Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You have reduced what you eat. You have kept up with exercise. The weight around your abdomen arrived sometime in the last year or two, and it is not responding the way weight usually responds when you make changes. It is not moving at the rate it should, if it is moving at all.
The most likely explanation is that the hormonal environment is working against you. Calorie balance still matters, but when cortisol is chronically elevated it changes where the body stores energy, disrupts the hormones that govern appetite and satiety, and reduces the effectiveness of the usual approaches. Applying only a calorie-focused solution to a pattern driven by a dysregulated stress response often produces minimal results and considerable frustration.
This post explains the specific hormonal mechanism that causes stress-related abdominal weight gain, why dietary restriction alone does not address it, and what actually changes the hormonal environment driving the storage.
BEFORE YOU READ FURTHER This post describes the cortisol-driven fat storage mechanism behind stress-related abdominal weight gain. This is a real and well-documented biological pathway. It is one mechanism behind weight gain, not the only one. If weight gain has been rapid, significant, or accompanied by other concerning symptoms including changes in vision, severe fatigue, significant changes in blood pressure, stretch marks appearing rapidly, or significant muscle weakness, please see a GP before attributing it to stress. These could indicate clinical hypercortisolism or other conditions requiring medical assessment. The content below is written for the common pattern of gradual abdominal weight gain during prolonged periods of chronic stress in otherwise healthy people. The mechanism described here is most relevant for people who notice weight accumulating specifically around the abdomen during or following a period of sustained stress, that is resistant to dietary changes that would normally produce results. If that describes your situation, read on. |
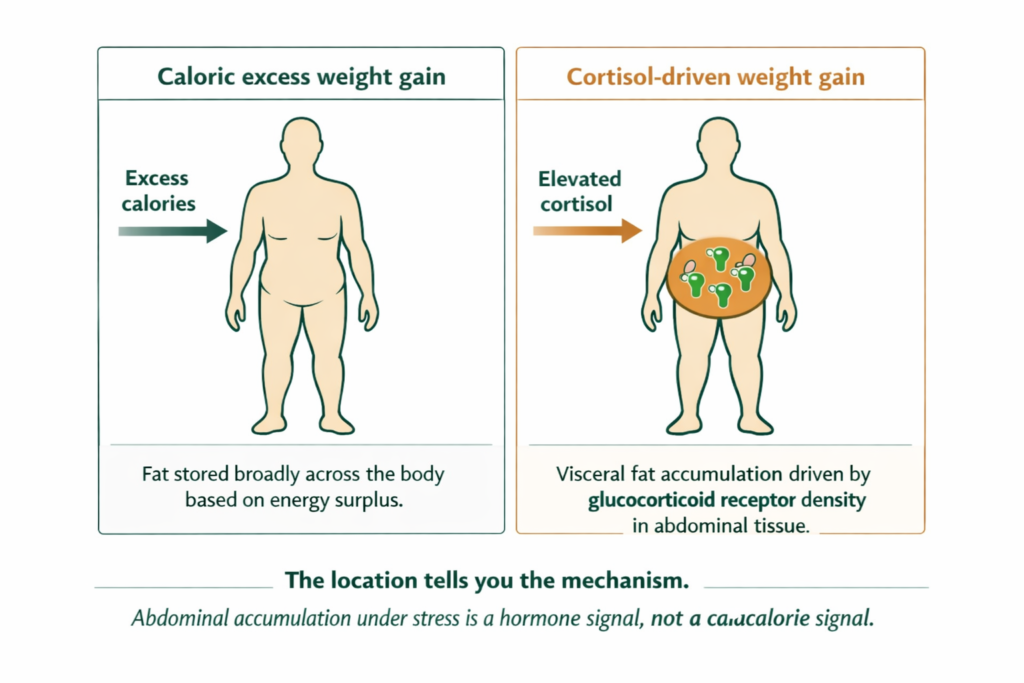
When cortisol is chronically elevated, it activates glucocorticoid receptors concentrated in visceral adipose tissue, the fat stored deep in the abdominal cavity around the organs. These receptors, when activated by cortisol, signal the body to preferentially store fat in that location. This is not a side effect of general weight gain. It is a targeted fat storage instruction sent directly to abdominal tissue by the hormone itself (Epel et al., 2000).
The mechanism has a biological rationale. In the context of acute survival stress, storing energy reserves near the core organs makes metabolic sense. The body is preparing for a crisis that requires rapid energy access. The problem is that modern sustained stress, work pressure, financial anxiety, relational difficulty, keeps this signal active continuously. The body stores fat in the abdominal region not once in response to a crisis but continuously in response to a stress state that never fully resolves.
Cortisol may also interact with sex hormone balance. Some researchers propose that sustained cortisol elevation influences the relative availability of progesterone and oestrogen through shared precursor pathways, with oestrogen relative excess contributing to fat storage in the abdomen, hips, and thighs. This is an area of active research and is not a mainstream clinical consensus. What is better established is that chronic stress disrupts the hormonal environment broadly through HPA axis dysregulation, sleep disruption, and insulin signalling changes, and this broader disruption contributes to the resistance to weight loss that many stressed people experience.
DEFINITION VISCERAL FAT Fat stored within the abdominal cavity, surrounding the internal organs rather than lying beneath the skin. Visceral fat is metabolically active and directly responsive to cortisol through glucocorticoid receptors concentrated in that tissue. Elevated cortisol does not cause general weight gain evenly distributed across the body. It causes preferential visceral fat accumulation in the abdominal region. This is why stress-related weight gain has a characteristic pattern of abdominal accumulation that is disproportionate to any changes in food intake. |
The full cortisol mechanism and how it produces this and other downstream effects is covered in our post on high cortisol symptoms and what the mineral depletion cycle does to your body.
Understanding that this is a hormonal storage signal rather than a caloric surplus changes what needs to be addressed. The next section explains what actually works.
This is the part most dietary advice misses entirely, and the reason people find themselves eating less and still not losing the abdominal weight.
Caloric restriction is itself a physiological stressor. When food intake drops significantly, the body interprets the energy deficit as a threat and increases cortisol output to mobilise energy reserves and sustain function. The very intervention intended to reduce the abdominal fat activates the hormone that is directing fat to that location. The cortisol signal intensifies.
This creates the pattern many people describe: eating carefully, exercising consistently, and finding the scale does not move or moves minimally. The body is receiving a stress signal from the dietary restriction that compounds the stress signal from the life circumstances driving the original cortisol elevation. Both are pointing at the same hormonal fat storage instruction.
Water retention adds another layer. Cortisol causes sodium retention through its interaction with aldosterone, the hormone that regulates fluid balance. Under sustained cortisol elevation, the body holds more water, particularly in the abdominal and facial regions. This is why people notice a puffy, bloated quality alongside the abdominal weight that does not respond to dietary changes. The water retention is hormonal, not dietary.
DOES THIS APPLY TO YOU? If your weight gain is specifically in the abdomen, arrived or worsened during a period of sustained stress, is resistant to dietary changes that would normally produce results, and is accompanied by other cortisol symptoms including poor sleep, afternoon energy crashes, or increased susceptibility to illness, the cortisol mechanism is almost certainly the primary driver. If weight gain is evenly distributed, directly proportional to changes in food intake, or not accompanied by the stress context, cortisol is less likely to be the primary mechanism and standard dietary and activity changes are more likely to produce results. |
Once the mechanism is clear, the solution hierarchy becomes straightforward. The stressor comes first. The biology is addressed in parallel.
The honest solution hierarchy follows the mechanism. Cortisol is the driver. Reducing cortisol is the primary lever. Everything else supports that primary action.
The glucocorticoid receptor signal that is directing fat to the abdomen is sent by cortisol. Cortisol is produced in response to sustained demand. Reducing that demand is the primary intervention. This is not always simple and it is not always immediately possible, but it is the direction the solution points. Dietary changes that do not reduce cortisol do not change the fat storage signal.
Where the sustained demand cannot be immediately reduced, genuine recovery windows matter. Not busy rest where the mind continues processing the stressor. Actual deactivation: time where the HPA axis receives minimal new activation input. Sleep quality improvement, parasympathetic activation through rest and movement that is genuinely restorative rather than another form of demand, and reducing secondary stressors where possible all support this primary direction.
Dietary composition matters significantly here, beyond total caloric intake. Refined carbohydrates and sugar produce blood glucose fluctuations that create additional cortisol spikes and compound the existing stress pattern. Reducing these is relevant both from a caloric standpoint and because of their effect on blood glucose stability and cortisol output. Adequate dietary protein supports satiety and reduces the physiological stress response that accompanies prolonged caloric restriction. Aggressive calorie restriction without dietary quality improvement often worsens the cortisol pattern.
Movement that reduces cortisol rather than adding to it: moderate, enjoyable physical activity rather than high-intensity training that produces its own cortisol spike. This is counterintuitive for people who have been told to exercise more to lose weight. In the context of chronic cortisol elevation, excessive high-intensity exercise can worsen the hormonal environment.
Sleep is the most powerful cortisol-regulating intervention available without medication. Cortisol follows a diurnal rhythm that is anchored to sleep-wake cycles. Consistently poor sleep disrupts that rhythm and maintains elevated baseline cortisol independently of external stressors. Improving sleep quality directly reduces the cortisol baseline driving fat storage.
While the primary work of reducing demand and improving sleep is underway, adaptogenic support addresses the stress response from the biological side. Ashwagandha has evidence from randomised controlled trials for reducing perceived stress and serum cortisol in adults under chronic stress. A well-cited trial found significant cortisol reductions over eight weeks of standardised ashwagandha extract versus placebo (Chandrasekhar et al., 2012). The mainstream medical system does not typically recommend supplements for stress management, not because the evidence is absent but because it falls outside the disease treatment model. For someone managing chronic stress in the context it is described here, the evidence base is relevant and worth knowing about.
Magnesium has a well-documented relationship with the stress response. Research suggests it plays a role in HPA axis regulation, and magnesium levels fall under chronic stress through increased urinary excretion. Lower magnesium availability may contribute to a more reactive stress response and slower cortisol recovery. This is a compounding factor that operates alongside the primary demand load. Restoring magnesium through more bioavailable forms, whether ionic magnesium in the morning sipping protocol or standard magnesium glycinate or citrate, addresses this mineral side of the stress pattern while the primary demand reduction work is proceeding.
WHAT TO DO ABOUT IT The most effective approach to stress weight gain works in the correct order. Reduce the stressor load first: this is the primary driver and no hormonal support changes the fat storage signal while the cortisol elevation is being continuously sustained. Support the hormonal environment through sleep prioritisation, movement that genuinely restores rather than stresses, and dietary composition that avoids blood glucose spikes. Support the biological recovery layer in parallel with ionic mineral restoration and adaptogenic HPA axis support. Caloric restriction is not the primary tool here and aggressive restriction will compound the cortisol signal. The goal is hormonal normalisation, not caloric deficit. |
DOES THIS APPLY TO YOU? If you have addressed the stressor load genuinely and sleep is reasonably managed and the abdominal weight is still not shifting after eight to twelve weeks, the broader hormonal picture including progesterone and oestrogen balance may be worth investigating. The low progesterone post covers the hormonal weight pattern specifically and is the relevant next step for women experiencing this alongside cycle-related symptoms. |
The progesterone-oestrogen mechanism behind abdominal fat storage is covered in full in our post on low progesterone symptoms and why the same hormonal problem produces so many different effects.

Standard Thinking | The Biological Reality |
|---|---|
Eat less and you will lose the stress weight | Cortisol-driven abdominal fat responds to cortisol reduction, not caloric reduction. Aggressive caloric restriction increases cortisol and can compound the fat storage signal rather than reversing it |
Exercise more to burn the stress weight off | Restorative moderate movement reduces cortisol. High-intensity training produces its own cortisol spike. The type of movement matters more than the volume when cortisol is the mechanism |
Stress weight gain is just emotional eating | Cortisol directly activates glucocorticoid receptors in visceral abdominal tissue and signals preferential fat storage there regardless of food intake. The mechanism is hormonal, not behavioural |
It will go away when the stressful period ends | The stressor ending removes the primary driver but does not reverse the accumulated fat already stored under the glucocorticoid signal. Active hormonal restoration is required for that to shift |
This is just bloating, not real weight gain | Water retention from cortisol-aldosterone interaction is real and adds visible abdominal volume. But visceral fat accumulation from glucocorticoid receptor activation is also real and requires different management from fluid retention |
Research supports an association between chronically elevated cortisol and preferential abdominal fat accumulation. Visceral adipose tissue has a higher concentration of glucocorticoid receptors, which may make it more responsive to cortisol signalling. Chronic stress also disrupts insulin sensitivity, sleep quality, and appetite regulation, all of which contribute to weight gain independently. The relationship is well-documented as an association. The precise mechanism involves multiple interacting systems rather than cortisol acting alone. The broader hormonal disruption from chronic stress, not a single pathway, is what makes stress-related abdominal weight gain resistant to standard calorie restriction.
Glucocorticoid receptors, which respond to cortisol, are more densely concentrated in visceral abdominal tissue than in other fat depots. When cortisol is chronically elevated, it activates these receptors and signals that specific tissue to preferentially accumulate fat. The body is responding to a perceived survival threat by building energy reserves near the core organs. The biological mechanism is precise and location-specific, not a general weight gain effect.
Caloric restriction alone is an ineffective primary strategy for stress-related abdominal weight gain because it does not address the cortisol signal driving the fat storage. Aggressive caloric restriction can compound the problem by raising cortisol through the physiological stress of the energy deficit itself. The most effective approach reduces the demand driving cortisol elevation, supports sleep and restorative movement to lower the cortisol baseline, and uses dietary composition to reduce blood glucose spikes that worsen the cortisol signal. Caloric balance matters but it is not the primary lever here.
The timeline depends primarily on how quickly the cortisol baseline reduces. In people who address the stressor load, improve sleep, and support the biological recovery layer, measurable improvement in abdominal fat distribution typically begins over eight to twelve weeks of sustained cortisol normalisation. Water retention from cortisol-aldosterone interaction resolves faster, often within two to three weeks of cortisol improvement. The visceral fat accumulated under the glucocorticoid signal takes longer as the body redistributes stored energy once the hormonal instruction to accumulate it has changed.
Yes, through its interaction with aldosterone, the hormone that regulates fluid and sodium balance. Elevated cortisol stimulates aldosterone, which causes sodium and water retention particularly in the abdominal and facial regions. This is why stress-related abdominal weight often has a bloated, puffy quality alongside the actual fat accumulation. Water retention from this mechanism responds to cortisol reduction rather than to changes in fluid or sodium intake.
ONE MORE THING BEFORE YOU GO If you have been eating well, exercising, and the weight around your abdomen is still not shifting, leave it in the comments below. Tell us how long it has been happening and whether it coincided with a period of sustained stress. We read every comment and respond with what the research says about your specific pattern. If you have already addressed the stress side and the weight is still not moving, that is a more specific question and we will answer it directly rather than giving you a generic response. |
Legal Disclaimer The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are experiencing persistent sleep disruption or significant anxiety, consult a qualified healthcare provider.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!




No products in the cart.