Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You feel relatively normal for most of the month. Then, somewhere in the week or ten days before your period, the energy disappears. You are exhausted in a way that feels different from ordinary tiredness. You sleep and do not feel better. Your brain slows down. Your muscles feel heavy. And then your period arrives and within a day or two, you feel like yourself again.
This happens every month. You have probably been told it is just PMS. It is not.
What you are experiencing is a specific and predictable biological event. Three overlapping mechanisms converge in the late luteal phase and produce the fatigue, sleep disruption, and cognitive fog that disappear when your period begins. This post explains exactly what those mechanisms are and what you can do about them.
BEFORE YOU READ FURTHER Severe premenstrual fatigue is a recognised symptom of Premenstrual Dysphoric Disorder (PMDD), a clinical condition affecting approximately 3 to 8 percent of women of reproductive age. PMDD is distinguished by symptoms that are present in the luteal phase and resolve after the onset of menses across most cycles, with a symptom-free period in the follicular phase. If your premenstrual fatigue is severe enough to significantly impair your ability to work, maintain relationships, or function daily, please raise PMDD specifically with your GP rather than self-managing. If your premenstrual fatigue is significant but not functionally disabling, the functional mechanisms described below are common, frequently overlooked, and often modifiable without clinical diagnosis. |
Mark how many of these apply in the seven to ten days before your period
DOES THIS APPLY TO YOU? If six or more of these apply consistently in the premenstrual window and resolve within one to two days of your period starting, the luteal phase mechanism described below is a high-probability primary driver. The key diagnostic signal is the pattern itself: consistent onset in the same cycle window and consistent resolution within two days of menstruation beginning. |
Progesterone peaks around day 21 of a typical 28-day cycle and then declines rapidly in the days before menstruation. What matters here is not progesterone itself but what happens to its primary metabolite, allopregnanolone.
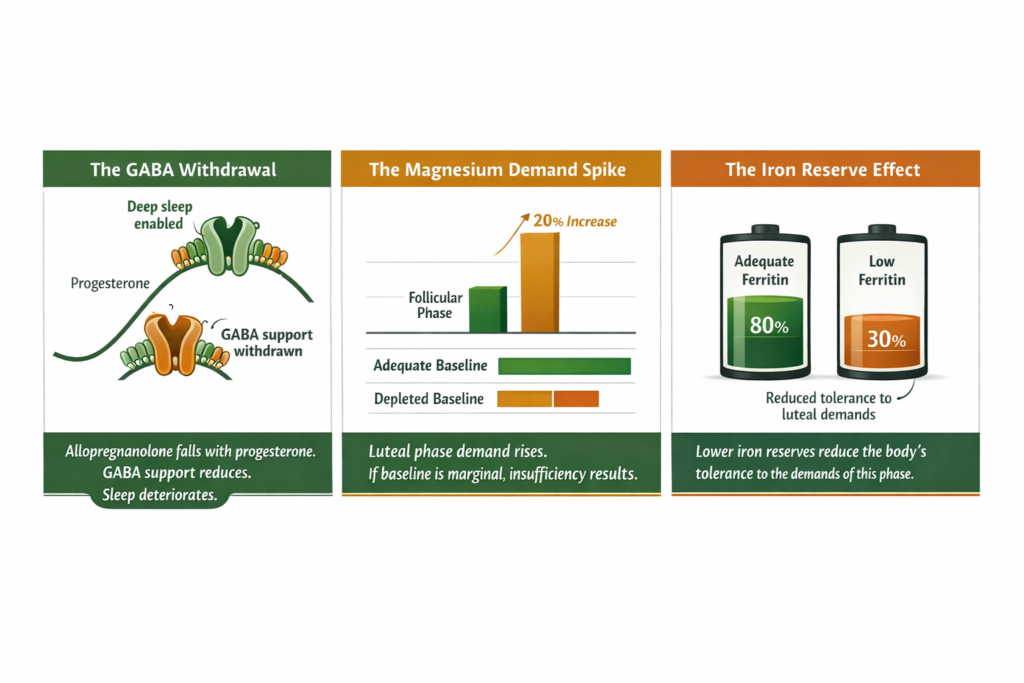
Allopregnanolone is a potent positive allosteric modulator of GABA-A receptors, the brain’s primary inhibitory receptors that govern nervous system calm, deep sleep initiation, and anxiety regulation. When allopregnanolone is high, the nervous system is calm and sleep is deep. When it drops as progesterone falls in the late luteal phase, this GABA support withdraws rapidly.
It is worth noting that sensitivity to allopregnanolone fluctuations varies between women. Some experience the withdrawal as a significant shift in sleep quality, mood, and energy. Others notice a milder effect. The mechanism is consistent but the subjective experience of it is not uniform.
The result in those who are sensitive is a nervous system that loses a significant source of inhibitory tone within a short window. Sleep architecture deteriorates. Deep sleep stages shorten. The nervous system runs hotter. You feel exhausted because your cells need the restoration that deep sleep provides, and the mechanism that enables deep sleep has just been significantly reduced.
This is not a mood disorder. It is a neurotransmitter event driven by hormonal withdrawal.
Magnesium demand increases in the luteal phase. Progesterone synthesis itself requires magnesium. The cortisol output that accompanies the luteal phase stress response depletes cellular magnesium. And the GABA receptor function that allopregnanolone supports also requires magnesium as a cofactor.
If your baseline cellular magnesium is already marginal, the increased demand in the late luteal phase pushes it into insufficiency. The consequences compound the progesterone drop: further GABA receptor impairment, disrupted sleep architecture, increased muscle tension and heaviness, increased cortisol sensitivity, and reduced ATP production from the mitochondrial magnesium dependency.
Research consistently associates lower magnesium status with more severe premenstrual symptoms including fatigue, mood changes, and sleep disruption. The relationship is mechanistic rather than incidental.
Each menstrual cycle involves 30 to 80ml of blood loss, which carries iron out of the body. In women whose ferritin levels are already low or borderline, this monthly loss compounds over time. Women with lower iron reserves have reduced cellular energy production capacity, and symptoms commonly occur at lower ferritin levels despite laboratory reference ranges appearing normal.
Iron is required for the electron transport chain, the process that produces the majority of cellular ATP. When iron stores are marginal, the demands of the late luteal phase — increased cortisol, disrupted sleep, elevated magnesium requirement — all place additional strain on an already-insufficient cellular energy picture.
Women with lower ferritin levels are substantially more likely to experience severe premenstrual fatigue than those with adequate stores. The two mechanisms, reduced iron reserve and luteal phase hormonal withdrawal, amplify each other.
The resolution is as mechanistically specific as the onset.
When menstruation begins, progesterone and allopregnanolone levels have already bottomed out. The withdrawal is complete. Over the following days, as the follicular phase begins, oestrogen starts to rise. Oestrogen has independent energising effects and also stimulates new mitochondrial biogenesis. The GABA receptor environment stabilises at its new baseline. Cortisol begins its follicular phase decline.
The rapid improvement many women feel in the one to two days after their period starts is not coincidental. It is the nervous system re-stabilising after the hormonal withdrawal event has completed.
This cycle repeating every month without improvement is not inevitable. It is a signal that the underlying mechanisms are not being addressed.
For the broader context of female fatigue and how the hormonal cycle interacts with cellular energy, see our post on why female fatigue follows a specific cyclical pattern and what the biology behind it actually is.
STEP 1 — CONFIRM THE PATTERN IS LUTEAL PHASE SPECIFIC
STEP 2 — ESTABLISH YOUR BASELINE IRON STATUS
STEP 3 — ADDRESS MAGNESIUM IN THE SECOND HALF OF YOUR CYCLE
STEP 4 — SUPPORT SLEEP ARCHITECTURE IN THE PREMENSTRUAL WINDOW
STEP 5 — REDUCE THE CORTISOL LOAD IN THE LUTEAL PHASE
The two inputs most directly relevant to the luteal phase mechanism are magnesium and cortisol support. Both address different aspects of the same GABA withdrawal event.
RESOLUTION CRITERIA: EVALUATE AFTER TWO FULL CYCLES
Track and rate daily for two cycles before starting. Compare at cycle two completion.
If two or more markers have improved across both evaluation cycles, the mechanism was the primary driver and the approach is working. Continue. If fewer than two markers have improved after two full cycles of consistent execution, escalate: hormonal panel with progesterone tested in the mid-luteal phase, typically seven days after confirmed ovulation, to account for cycle length variation. Discuss PMDD specifically with your GP if symptoms are functionally impairing. Request an intracellular mineral panel rather than standard serum testing.
WHAT THIS APPROACH WILL NOT FIX
This approach will not resolve PMDD, endometriosis-related fatigue, clinical iron deficiency anaemia, thyroid dysfunction, or autoimmune conditions that worsen premenstrually. In those cases this approach may support baseline function but is not a substitute for clinical assessment and treatment. If premenstrual fatigue is functionally disabling, clinical evaluation takes priority.
If this monthly crash has been a consistent feature of your cycle, it is not an inevitable consequence of being a woman. It is a biological pattern with three specific mechanisms and targeted interventions for each one. Track two cycles before starting, address the mechanisms in order, and evaluate against your baseline at cycle two.
Standard Thinking | The Biological Reality |
|---|---|
Premenstrual fatigue is just PMS | It is a predictable biological event driven by three overlapping mechanisms: allopregnanolone withdrawal, magnesium demand increase, and reduced iron reserve. These are often modifiable |
Taking the pill will fix it | Combined oral contraceptives suppress the natural hormonal cycle including the progesterone rise and fall. Some women find this reduces premenstrual symptoms. Others find it introduces a different hormonal pattern. It is a clinical decision not a first-line nutritional fix |
You just need to push through it | The GABA withdrawal mechanism means premenstrual fatigue is a neurotransmitter event not a motivation deficit. Pushing through compounds the cortisol load and worsens the mechanism |
Magnesium is just for cramps | Magnesium addresses the GABA receptor cofactor insufficiency, the cellular energy production deficit, and the sleep architecture disruption simultaneously |
The fatigue will improve with age | Without addressing the underlying magnesium depletion and iron insufficiency, the pattern typically worsens as progesterone declines naturally through the late 30s and into perimenopause |
Premenstrual fatigue is driven by three converging mechanisms in the late luteal phase. Progesterone drops and its metabolite allopregnanolone withdraws from GABA receptors, disrupting deep sleep and increasing nervous system arousal. Magnesium demand rises in the luteal phase and pushes cellular magnesium lower in women whose baseline is already marginal, further impairing GABA function and ATP production. And women with lower iron reserves have reduced cellular energy production capacity that makes the demands of this phase harder to tolerate. The combination produces the predictable monthly crash.
As women move through their 30s into perimenopause, progesterone begins a natural gradual decline. This means the drop in allopregnanolone in the late luteal phase becomes sharper relative to its starting point. Simultaneously, cumulative magnesium depletion from years of inadequate dietary intake compounds over time. The result is a premenstrual window that becomes progressively more symptomatic unless the underlying mineral and hormonal mechanisms are actively addressed.
Magnesium demand increases in the luteal phase for multiple reasons including progesterone synthesis, cortisol counterbalancing, and GABA receptor function. In women with borderline cellular magnesium, this increased demand pushes the system into insufficiency during the exact window that allopregnanolone is withdrawing from GABA receptors. Research consistently associates lower magnesium status with more severe premenstrual fatigue, sleep disruption, and mood symptoms. Addressing magnesium specifically in the second half of the cycle is the most targeted intervention for this mechanism.
The improvement is mechanistically specific. When menstruation begins, the allopregnanolone withdrawal event is complete. The nervous system stabilises at its new baseline. Over the following days the follicular phase begins, oestrogen rises with its independent energising effects, and cortisol begins its natural follicular decline. The rapid improvement is the resolution of the withdrawal event, not a coincidence.
Women with lower ferritin levels are substantially more likely to experience severe premenstrual fatigue. Iron is required for the electron transport chain, the process that produces the majority of cellular ATP. Lower iron reserves reduce the body’s tolerance to the additional demands of the late luteal phase. Symptoms commonly occur at lower ferritin levels despite laboratory reference ranges appearing normal. Requesting iron studies including ferritin from your GP is the appropriate first step. Clinical practice often treats ferritin below 50 micrograms per litre as insufficient in symptomatic patients even when haemoglobin is normal.
ONE MORE THING BEFORE YOU GO If your premenstrual fatigue pattern does not quite match what is described here, or if you have tried the correction approach and want to discuss what the next step might be, leave it in the comments below. Tell us which symptoms apply, where in your cycle they are worst, and whether the pattern is getting more severe over time. We read every comment and respond. |
Legal Disclaimer
The information in this post is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always seek personalised advice from a qualified healthcare provider before starting or changing any treatment or supplement regimen.
Never Miss any Updates From Blog!




No products in the cart.