Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
Your energy has dropped. Your muscles ache without obvious reason. Your brain is slower than it used to be. You are on a statin and your doctor says your bloods are fine. Or you are not on anything and still cannot explain why you feel like this.
CoQ10 deficiency is one of the frequently overlooked explanations for persistent fatigue, muscle symptoms, and cognitive decline. It is not included in standard blood panels. Most GPs do not test for it. And yet its role in cellular energy production is central to the point that when levels drop, the effects are felt throughout the entire body.
This post covers what CoQ10 deficiency symptoms actually look like, what causes CoQ10 to drop, and what a structured response involves.
BEFORE YOU READ FURTHER CoQ10 deficiency exists on a spectrum. Primary CoQ10 deficiency is a rare genetic condition requiring specialist management. Secondary CoQ10 deficiency, where levels have dropped due to medication, ageing, oxidative stress, or dietary insufficiency, is far more common and is what this post addresses. If you are experiencing severe muscle weakness, unexplained muscle breakdown, kidney involvement, or neurological symptoms, please see your GP promptly. These can indicate primary CoQ10 deficiency or other conditions requiring clinical investigation. If your fatigue, muscle symptoms, and cognitive complaints are persistent but not severe, and you are on a statin or over 40, the secondary deficiency mechanism described below is a plausible and frequently overlooked contributor worth investigating. |
Mark how many of the following apply consistently across months rather than days.
A useful self-sorting signal: CoQ10-related fatigue typically presents alongside muscle symptoms. Fatigue without muscle involvement is more often driven by sleep disruption, cortisol dysregulation, or iron-related mechanisms. If your fatigue is accompanied by muscle aching, weakness, or cramping, CoQ10 is a more specific candidate than if fatigue is the sole symptom.
DOES THIS APPLY TO YOU? If six or more of these apply and have been present for months, CoQ10 insufficiency is a relevant mechanism to evaluate, particularly if you are over 40, taking a statin, or under sustained psychological stress. If post-exertional malaise is prominent alongside unrefreshing sleep and cognitive symptoms lasting six months or more, raise ME/CFS specifically with your GP as a distinct possibility requiring specialist assessment. |
Statins work by blocking HMG-CoA reductase, an enzyme involved in cholesterol production. The same biochemical pathway that produces cholesterol also produces CoQ10. When you block that pathway, cholesterol production drops as intended. CoQ10 production drops alongside it.
Research consistently associates statin use with reduced CoQ10 levels. The symptoms that follow, muscle pain, fatigue, cognitive complaints, and reduced exercise tolerance, are among the most commonly reported statin side effects and overlap with symptoms associated with CoQ10 depletion. The mechanism includes CoQ10 depletion from blocking the shared biosynthetic pathway, alongside other mitochondrial effects.
Statin-associated muscle symptoms are multifactorial and not exclusively explained by CoQ10 depletion. But if you are on a statin and experiencing these symptoms, CoQ10 depletion is a mechanistically plausible contributor worth raising with your GP.
This does not mean statins should be avoided. The cardiovascular risk reduction evidence is strong. In some clinical guidelines in Europe and North America, CoQ10 supplementation alongside statin therapy is recommended for patients experiencing myopathy.
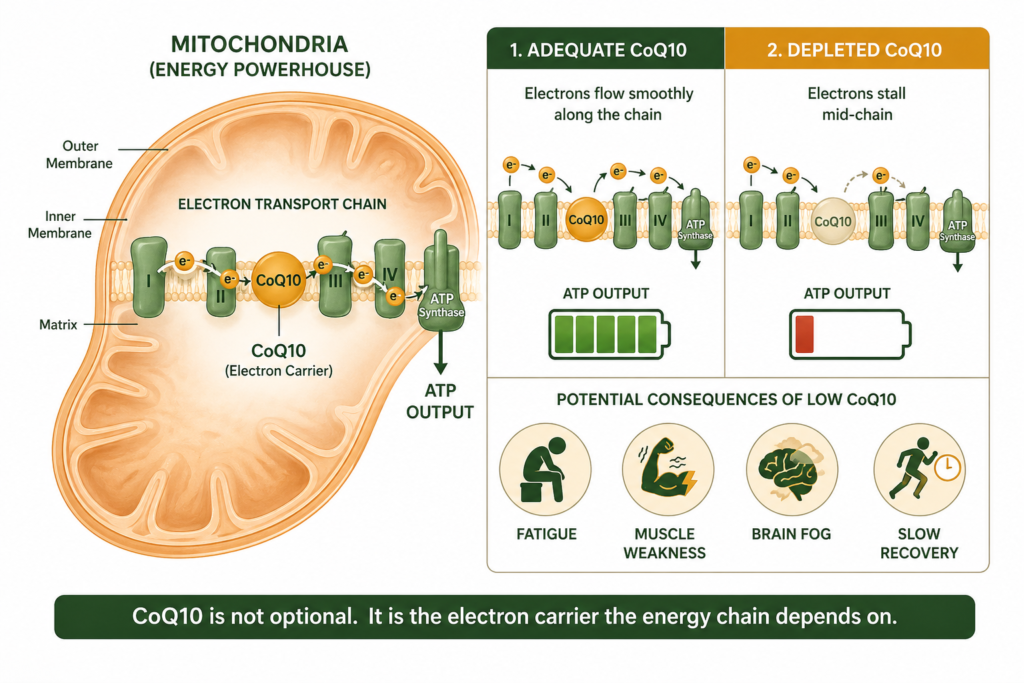
CoQ10 is a compound produced naturally in virtually every cell in the body. Its primary role is in the mitochondrial electron transport chain, the final stage of ATP production where the majority of cellular energy is generated. CoQ10 acts as an electron carrier, shuttling electrons through the inner mitochondrial membrane to drive ATP production. Without adequate CoQ10, this process slows, ATP output drops, and energy supply becomes insufficient for demand.
CoQ10 also functions as a fat-soluble antioxidant, protecting cell membranes and mitochondria from oxidative damage. This role connects CoQ10 status to cardiovascular health, brain function, and cellular ageing rate.
The connection between CoQ10 and fatigue is direct and biochemical rather than associative.
The electron transport chain uses electron carriers produced in earlier metabolic stages to generate the majority of cellular energy. CoQ10 is the molecule that accepts those electrons and passes them through the chain. Without adequate CoQ10, this transfer slows. The electron transport chain becomes a bottleneck. ATP production drops significantly.
The result is a body that cannot produce the energy it requires regardless of how much it rests, eats, or sleeps. The substrate is present. The process is compromised. This is why CoQ10-related fatigue fails to respond to the approaches that address ordinary tiredness.
Fatigue plus muscle symptoms together point more specifically toward mitochondrial energy insufficiency than toward cortisol dysregulation, iron deficiency, or sleep disruption alone. If muscle symptoms are absent, other mechanisms are more likely primary.
Fatigue that worsens with exercise rather than improving over time. In CoQ10-related mitochondrial fatigue, exercise often makes symptoms worse because physical demand exceeds the compromised energy production capacity.
Fatigue in a statin user where symptoms began or worsened after starting therapy. The timing makes CoQ10 depletion a mechanistically plausible contributor.
Fatigue over 40 without clear clinical cause after normal blood testing warrants CoQ10 consideration given the age-related production decline.
If this pattern matches, the correction approach below is structured specifically around these variables. If fatigue is present without muscle symptoms, the chronic fatigue cluster posts covering HPA axis and sleep architecture may be a better starting point.
For the broader fatigue picture and full correction protocol, see our post on why persistent fatigue is a cellular energy problem and what a structured correction looks like.
CoQ10 is present in food but dietary amounts are generally modest compared to endogenous production and supplemental doses used in research.
Average dietary CoQ10 intake is estimated at 3 to 6mg per day. Research studies typically use doses of 100 to 300mg per day. Dietary intake alone is unlikely to compensate for significant depletion in statin users, older adults, or those with high oxidative stress loads. Dietary improvement is relevant but supplementation is the more direct approach where deficiency is suspected.
STEP 1 – ESTABLISH WHETHER COQ10 DEPLETION IS LIKELY
|
STEP 2 – RAISE IT WITH YOUR GP
|
STEP 3 – SUPPLEMENTATION WITHIN RESEARCH-SUPPORTED RANGES
|
STEP 4 – ADDRESS CONCURRENT MITOCHONDRIAL CONSTRAINTS
|
STEP 5 – ADDRESS THE CONTRIBUTING FACTORS
|
STEP 6 – EVALUATE AT 8 WEEKS
|
Once the clinical basics are addressed and supplementation is under way, the mineral support layer that underpins mitochondrial function more broadly is worth building in parallel.
WHAT THIS APPROACH WILL NOT FIX This approach will not resolve fatigue caused by untreated thyroid disease, anaemia, sleep apnoea, active infection, or diagnosed ME/CFS. In those cases, CoQ10 support may contribute to baseline function but is not a substitute for medical treatment. Clinical exclusion of these conditions is the appropriate first step before attributing fatigue to CoQ10 depletion. |
Standard Thinking | The Biological Reality |
|---|---|
CoQ10 is just a general wellness supplement | CoQ10 is required for the electron transport chain that produces the majority of cellular ATP. Its insufficiency directly impairs energy production at the biochemical level |
Normal blood tests mean you are not deficient | CoQ10 is not included in standard blood panels. Normal results do not address CoQ10 status |
Statins cause muscle pain through inflammation | The mechanism includes CoQ10 depletion from blocking the shared biosynthetic pathway, alongside other mitochondrial effects. Statin-associated muscle symptoms are multifactorial |
Diet alone can maintain CoQ10 levels | Average dietary intake is 3 to 6mg per day. Research doses are 100 to 300mg. Diet supports but cannot compensate for significant depletion |
Ubiquinol and ubiquinone are interchangeable | Ubiquinol has higher bioavailability, particularly in older adults where conversion from ubiquinone becomes less efficient |
CoQ10 deficiency produces a characteristic cluster including fatigue that does not resolve with rest, muscle weakness and aching without musculoskeletal explanation, reduced exercise tolerance with slow recovery, and cognitive symptoms including brain fog and reduced mental clarity. In statin users, these symptoms often appear or worsen after starting therapy. The pattern of fatigue plus muscle symptoms together is the most specific indicator pointing toward mitochondrial energy insufficiency as a contributor.
CoQ10 does not produce energy directly. It is an essential component of the electron transport chain that produces ATP. When CoQ10 is depleted, ATP production slows and fatigue results. Restoring adequate CoQ10 does not create energy above baseline. It restores the capacity that depletion has reduced.
The highest dietary sources are organ meats including beef heart and liver at 3 to 4mg per 100g, oily fish including sardines, mackerel, and salmon at 1 to 2mg per 100g, and beef and pork muscle meat at 1 to 3mg per 100g. Plant sources contain trace amounts. Average daily dietary intake is 3 to 6mg, significantly below the doses used in research on fatigue outcomes.
Statins block the HMG-CoA reductase pathway required for both cholesterol and CoQ10 production. Research consistently associates statin use with reduced CoQ10 levels. The mechanism includes CoQ10 depletion alongside other mitochondrial effects. Statin-associated muscle symptoms are multifactorial. If you are on a statin and experiencing muscle pain or fatigue, raising CoQ10 specifically with your GP is appropriate. In some clinical guidelines, CoQ10 supplementation alongside statin therapy is recommended for patients experiencing myopathy.
Research studies typically run 8 to 12 weeks before measuring outcomes. Cellular CoQ10 replenishment is gradual. Expecting results within one to two weeks leads to premature discontinuation. Evaluating at 8 weeks against specific markers, exercise tolerance, muscle comfort, cognitive clarity, morning energy, and daily energy stability, gives a reliable signal of whether supplementation is addressing the right mechanism.
ONE MORE THING BEFORE YOU GO If your symptom pattern does not quite match what is described here, or if you are on a statin and trying to work out whether CoQ10 depletion is contributing to what you are experiencing, leave it in the comments. Tell us which symptoms apply, how long they have been present, and whether you are on any relevant medication. We read every comment and respond with what the research says about your specific situation. |
Legal Disclaimer
The information in this post is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always seek personalised advice from a qualified healthcare provider before starting or changing any treatment or supplement regimen, particularly if you are taking statin medications, anticoagulants, or other prescription medications.
If this pattern matches your experience, the next step is not more trial and error. It is structured evaluation. Confirm clinical basics through GP assessment, assess likelihood based on your risk factors, implement a defined CoQ10 trial within established ranges, and measure the outcome at 8 weeks. The 8-week outcome determines whether CoQ10 is a relevant driver.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!




No products in the cart.