Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You sleep eight hours. Sometimes nine. You go to bed at a reasonable time. You do not feel anxious about sleep. And yet you wake up exhausted, drag yourself through the morning on caffeine, and feel like you never went to bed at all.
This is usually not a sleep quantity problem. For most people in this pattern, the problem is not how many hours you are spending in bed. It is what is happening during those hours.
This post explains the specific biological mechanisms behind unrefreshing sleep, what is preventing your body from restoring itself overnight, and what a structured correction looks like.
BEFORE YOU READ FURTHER Unrefreshing sleep is one of the diagnostic criteria for ME/CFS. If you have experienced unrefreshing sleep alongside post-exertional malaise, cognitive impairment, and orthostatic intolerance for six months or more, please raise ME/CFS specifically with your GP rather than self-managing. Sleep apnoea also produces unrefreshing sleep and is underdiagnosed. If you snore, wake with headaches, or have been told you stop breathing during sleep, GP assessment and a sleep study are the appropriate first step before addressing the mechanisms below. If your sleep tests and blood panels are normal and you still wake exhausted, the functional mechanisms described below are common and frequently overlooked contributors worth investigating. |
Mark how many of these apply consistently across months rather than days.
DOES THIS APPLY TO YOU? If six or more of these apply consistently across months, the sleep architecture mechanism is a high-probability driver worth investigating. If the 2 to 4am waking is present alongside the exhausted morning pattern, cortisol rhythm disruption is a specific and plausible primary contributor. These patterns, particularly unrefreshing sleep alongside post-exertional malaise and cognitive symptoms lasting six months or more, should be raised with your GP as potential ME/CFS criteria. |
Sleep quality and sleep quantity are separate variables. Eight hours of shallow fragmented sleep is not equivalent to six hours of deep restorative sleep. The number of hours in bed tells you almost nothing about what those hours are doing for your body.
Cellular restoration, mitochondrial repair, hormonal recalibration, immune consolidation, and memory processing all occur primarily in specific sleep stages, particularly slow-wave deep sleep and REM sleep. If you are spending time in bed but not reaching or sustaining these stages, the restoration simply does not happen. You accumulate the equivalent of unpaid cellular debt every night.
Sleeping longer does not pay the debt. It keeps the debt accumulating at the same rate for more hours.
Three common functional mechanisms drive unrefreshing sleep when clinical causes are excluded.
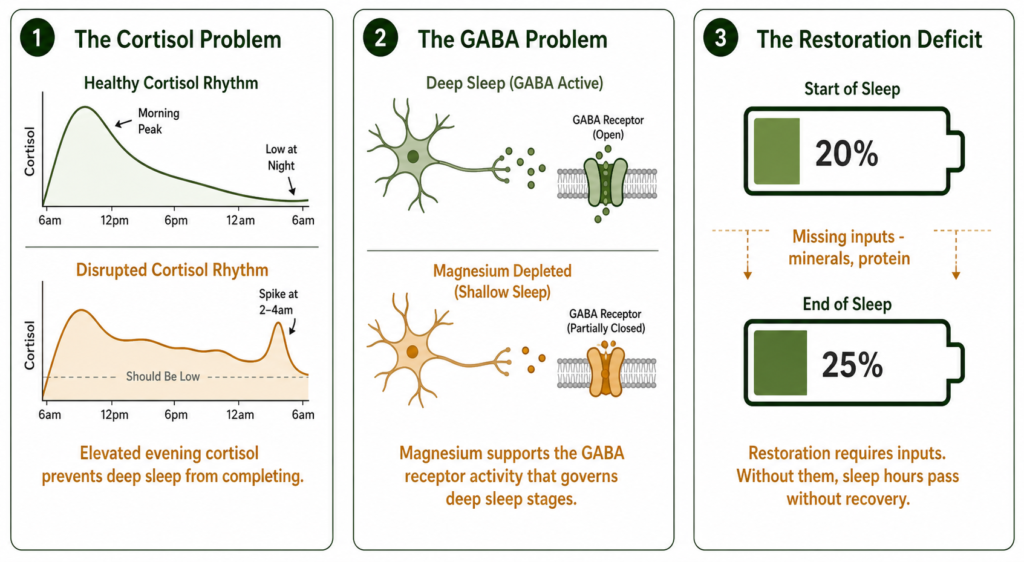
Cortisol follows a circadian rhythm, peaking in the early morning to prepare the body for waking and falling through the day to allow sleep. In people with sustained psychological stress or HPA axis dysregulation, this rhythm is disrupted. Cortisol remains elevated into the evening, preventing the full transition into deep sleep. It may spike in the middle of the night, producing the 2 to 4am waking pattern.
This is why sustained stress does not just make you anxious during the day. It actively fragments your sleep at night and prevents the deep restoration stages from completing. The nervous system remains in a low-level arousal state that never fully switches off.
GABA is the brain’s primary inhibitory neurotransmitter. It governs the transition from wakefulness into deep sleep and the maintenance of deep sleep stages. When GABA signalling is insufficient, the nervous system cannot sustain the inhibitory state required for deep sleep. Sleep becomes shallow, easily disrupted, and non-restorative even when duration is adequate.
Magnesium is directly involved in GABA receptor function. Research associates lower cellular magnesium status with reduced GABA activity and disrupted sleep architecture. This is the specific mechanism behind the restless activated waking pattern, the inability to stay in deep sleep, and the unrefreshed waking state that sleep duration alone does not explain.
Progesterone also modulates GABA receptors, which is why women in perimenopause frequently develop unrefreshing sleep even when sleep duration has not changed.
The body’s cellular repair and mitochondrial restoration processes require specific inputs during sleep. If the raw materials for this restoration, primarily magnesium, adequate protein, and electrolyte hydration, are insufficient, the repair process is incomplete regardless of how many hours are available. The battery spends the time connected but wakes with the same charge deficit it started with.
For the broader energy and fatigue context, see our post on why persistent fatigue is a cellular energy problem and what a structured correction looks like.
The 2 to 4am waking is one of the most diagnostically specific patterns in this cluster and almost no consumer health content explains it at the mechanism level.
This timing corresponds to the natural cortisol nadir, the lowest point in the circadian cortisol cycle. In people with HPA axis dysregulation, the rebound from this low point produces a cortisol spike that wakes the nervous system before the next sleep cycle can complete. The result is waking at 2 to 4am feeling alert or mildly anxious, lying awake for an hour or two, then falling back to sleep just before the alarm and waking exhausted.
If this pattern is familiar, cortisol rhythm disruption is a plausible primary driver. The correction approach below targets this specifically through Step 2.
Insomnia is difficulty falling or staying asleep. Unrefreshing sleep is sleeping without restoration. They are different problems with different mechanisms and different solutions.
Insomnia typically responds to sleep hygiene, cognitive approaches, and sometimes medication targeting sleep onset. Unrefreshing sleep does not respond to these because the problem is not sleep initiation. Standard sleep hygiene advice helps but does not address the cortisol rhythm, GABA insufficiency, or mineral depletion that prevent restorative deep sleep from occurring.
If you have tried sleep hygiene consistently and it has not resolved the unrefreshed waking, the functional mechanisms above are the more likely primary driver.
STEP 1 – EXCLUDE CLINICAL CAUSES FIRST
|
STEP 2 – ADDRESS THE CORTISOL RHYTHM
|
STEP 3 – SUPPORT THE GABA SLEEP MECHANISM
|
STEP 4 – ADDRESS THE MITOCHONDRIAL RESTORATION DEFICIT
|
The two inputs most directly relevant to both the GABA mechanism and the overnight mineral restoration are magnesium and the stress regulation layer. Both can be supported in parallel.
RESOLUTION CRITERIA: EVALUATE AT 4 WEEKS Record your baseline for 3 days before starting. Compare at day 28.
|
If two or more markers have improved at four weeks, the sleep architecture mechanism was a primary contributor. Continue the protocol. If fewer than two have improved after four weeks of consistent execution, do not continue the same approach. Escalate: request a formal sleep study to assess sleep architecture directly, and an intracellular mineral panel rather than standard serum testing.
WHAT THIS PROTOCOL WILL NOT FIX This approach will not resolve unrefreshing sleep caused by untreated sleep apnoea, primary insomnia disorder, medication side effects, active depression, or ME/CFS. In those cases this approach may support sleep quality at the margins but is not a substitute for clinical management. Step 1 clinical exclusion is not optional. |
Standard Thinking | The Biological Reality |
|---|---|
Sleeping more will fix tiredness on waking | Sleep quantity and sleep quality are separate variables. More hours of shallow sleep does not produce the restoration that deep sleep provides |
If you can fall asleep you do not have a sleep problem | Falling asleep easily and sleeping restoratively are different. Unrefreshing sleep is a sleep quality problem, not a sleep initiation problem |
Sleep hygiene is all you need | Sleep hygiene addresses sleep behaviours. It does not address cortisol rhythm disruption, GABA insufficiency, or mineral depletion that prevent restorative sleep stages from completing |
Alcohol helps you sleep | Alcohol suppresses deep sleep and REM stages while appearing to help with sleep onset. It is one of the most consistent producers of the unrefreshing sleep pattern |
Magnesium is a general supplement | Magnesium is directly involved in GABA receptor function that governs deep sleep architecture. Its insufficiency is associated with the specific unrefreshed waking pattern this post describes |
Waking unrefreshed after adequate sleep hours indicates that the restorative processes occurring during deep sleep stages are not completing effectively. The most common functional drivers are cortisol rhythm disruption preventing deep sleep from sustaining, GABA insufficiency from cellular magnesium depletion causing shallow fragmented sleep, and mitochondrial restoration deficit from insufficient mineral inputs. These are distinct from sleep duration issues and do not improve with more hours in bed.
Unrefreshing sleep has multiple possible causes. Clinical causes including sleep apnoea, ME/CFS, depression, hypothyroidism, and medication effects require clinical assessment. Functional causes where clinical testing returns normal results commonly include HPA axis cortisol rhythm disruption, GABA signalling insufficiency from magnesium depletion, and mitochondrial restoration deficit from inadequate cellular mineral status.
The 2 to 4am waking pattern corresponds to the natural cortisol nadir in the circadian rhythm. In people with HPA axis dysregulation, the rebound from this low point produces a cortisol spike that wakes the nervous system. The result is alert waking at this specific window, often with mild anxiety, followed by difficulty returning to sleep. This pattern is associated with cortisol rhythm disruption rather than a general sleep problem and responds specifically to the cortisol rhythm correction in Step 2.
Research associates magnesium with GABA receptor activity, which governs the transition into and maintenance of deep sleep stages. Lower cellular magnesium status is associated with disrupted sleep architecture including the shallow fragmented sleep that produces unrefreshed waking. Magnesium taken before bed specifically targets the sleep architecture mechanism rather than sleep onset. Forms with higher bioavailability are generally preferred in research contexts. This is not a sedative effect. It is support for the neurological mechanism that enables restorative sleep.
When the primary mechanism is cortisol rhythm disruption or GABA insufficiency from magnesium depletion, measurable improvement in waking energy and sleep quality can begin within two to four weeks of consistent protocol execution. The wake time consistency intervention can show results within seven to ten days. Evaluating at four weeks against a recorded three-day baseline gives an objective signal of whether the approach is addressing the correct mechanism.
ONE MORE THING BEFORE YOU GO If your waking pattern does not quite match what is described here, or if you have tried the protocol and want to talk through the next step, leave it in the comments below. Tell us how long the pattern has been present, whether the 2 to 4am waking applies, and which mechanisms you have already addressed. We read every comment and respond with what the research says about your specific situation. |
Legal Disclaimer
The information in this post is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Unrefreshing sleep has many possible causes. Always seek personalised advice from a qualified healthcare provider before starting or changing any treatment or supplement regimen.
If you are sleeping enough hours but waking exhausted, more sleep is not the answer. The answer is restoring the biological conditions that allow sleep to be restorative. Fix the cortisol rhythm, support the GABA mechanism, and provide the mineral inputs that overnight restoration requires. Measure the outcome at four weeks. The result tells you whether you have been addressing the correct variable.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!




No products in the cart.