Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You are tired in a way that sleep does not fully fix. You might have noticed your hair thinning. Your hands and feet are cold when they should not be. Your legs are restless at night. You cannot concentrate the way you used to.
These symptoms often share a common cause. In many people experiencing this cluster, the thread connecting them is insufficient iron reaching the cells that need it.
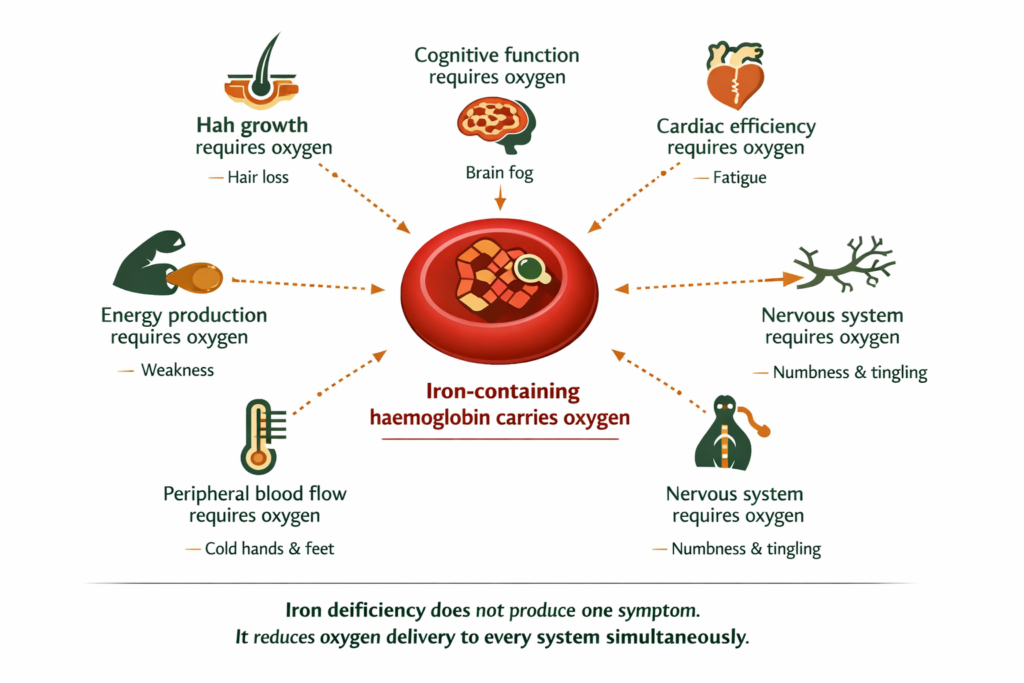
Iron is what makes haemoglobin. Haemoglobin is what carries oxygen in your blood. When iron is low, every cell in your body receives less oxygen than it needs to function. Fatigue is the obvious result. But the oxygen deficit affects your hair follicles, your temperature regulation, your nervous system, your heart rate, and your cognitive function simultaneously. That is why low iron produces such a wide and seemingly unrelated symptom cluster.
This post goes through each one. By the end you will know whether the picture fits and what to do about it.
DEFINITION WHAT ARE SYMPTOMS OF LOW IRON The most commonly reported symptoms of iron deficiency include persistent fatigue that does not resolve with rest, increased hair shedding, cold hands and feet, restless legs at night, pale inner eyelids, brain fog, heart palpitations, and shortness of breath on light exertion. These symptoms reflect reduced oxygen delivery to tissues from insufficient haemoglobin production. |
BEFORE YOU READ FURTHER This post covers the symptoms and mechanisms of low iron and iron deficiency. The symptoms described are real and well-documented. Iron deficiency is one of the most common nutritional deficiencies globally. If your symptoms are severe, came on rapidly, or include significant shortness of breath at rest, chest pain, or you are pregnant, please see a GP before pursuing a self-directed approach. These presentations need clinical assessment and may require prescribed iron treatment. If your symptoms have been building gradually over weeks to months, particularly during or after periods of high demand, significant blood loss including heavy periods, or a long period of low dietary iron intake, this post is written for your situation. |
Mark the ones that apply. You do not need all of them.
Fatigue that does not resolve with rest. You sleep and still feel unrestored. The tiredness is persistent rather than situational.
Hair thinning or increased shedding. More hair in the shower, on your pillow, or in your brush than you used to notice.
Cold hands and feet. Your extremities feel cold in conditions where other people are comfortable. Sometimes cold all over.
Restless legs at night. An uncomfortable urge to move your legs when you are trying to sleep. Often worse at night, better with movement.
Pale skin or pale inner eyelids. The inside of your lower eyelid looks lighter pink or white rather than deep red.
Brain fog and poor concentration. Slower thinking, difficulty holding a train of thought, or feeling mentally flat.
Heart palpitations. Awareness of your heartbeat, occasional racing or fluttering, particularly during light physical activity.
Shortness of breath on exertion. Getting breathless doing things that did not previously wind you. Climbing stairs, walking quickly.
Brittle nails or spoon-shaped nails. Nails that break easily, or have developed a concave, spoon-like shape.
Headaches. Persistent low-grade headaches without an obvious cause.
If four or more of these are present consistently, particularly in the context of heavy periods, low dietary iron, or a period of high physiological demand, iron deficiency is worth investigating. The sections below explain the mechanism and how to distinguish the iron pattern from thyroid and other common causes.
Iron deficiency affects a significant proportion of women of reproductive age globally, making it one of the most frequently overlooked causes of the fatigue and hair loss pattern described above.
If this pattern fits: the next section explains the mechanism and what to test first.
Iron sits inside haemoglobin, the protein in red blood cells that binds oxygen in the lungs and delivers it to every tissue in the body. Without enough iron, the body produces fewer or smaller red blood cells with less haemoglobin. Less haemoglobin means less oxygen delivered per unit of blood.
The body responds to this by prioritising which organs receive the most oxygen. The heart, brain, and core organs are prioritised. Peripheral blood flow to the hands, feet, and skin is reduced. Hair follicles, which are non-essential to immediate survival, receive less. Cognitive function and energy production, which are oxygen-intensive processes, slow down. Temperature regulation, which depends on adequate peripheral blood flow, becomes less effective.
In the context of iron deficiency, many of these symptoms can trace to the same oxygen delivery deficit expressing itself across different tissues. The hair loss, the cold hands, the brain fog, the fatigue, the restless legs often reflect the same underlying mechanism, though other causes can produce each symptom independently.
DEFINITION HAEMOGLOBIN A protein inside red blood cells that contains iron and binds oxygen molecules. Haemoglobin picks up oxygen in the lungs and releases it to tissues throughout the body. When iron is insufficient, the body cannot produce adequate haemoglobin. Red blood cells become smaller and carry less oxygen per cell. The resulting oxygen deficit affects every tissue in the body proportionally to how much oxygen that tissue requires to function. Energy-intensive tissues like the brain and muscles are affected most, but all tissues are affected to some degree. |
Understanding why all the symptoms connect to the same mechanism makes it easier to recognise whether the pattern applies to you. Each section below covers one expression of that mechanism.
Muscle cells produce energy through a process that requires oxygen. When oxygen delivery falls, energy production falls with it. The fatigue of iron deficiency is not tiredness from lack of sleep. It is cellular energy production running below its capacity because the fuel supply has been reduced.
This is why iron deficiency fatigue has a particular quality: it does not respond fully to rest. You can sleep well and still feel unrestored, because the energy deficit is happening at the cellular level, not at the sleep-debt level. The battery is not charging properly regardless of how long you leave it plugged in.
The fatigue is often accompanied by breathlessness on light exertion, because the cardiovascular system is compensating for reduced oxygen delivery per red blood cell by increasing heart rate and breathing rate. Climbing stairs, walking quickly, or carrying anything heavier than usual produces disproportionate breathlessness. This is the heart working harder to move more blood faster to compensate for each unit of blood carrying less oxygen.
WHAT TO DO ABOUT IT If fatigue and breathlessness on exertion are your primary symptoms, a full blood count with ferritin is the correct first step. Ask specifically for ferritin, not just haemoglobin. Ferritin measures stored iron. Haemoglobin can still be in the low-normal range while ferritin is significantly depleted, which is the pre-anaemic state where symptoms are often already present. Addressing the iron deficit at the ferritin stage, before anaemia develops, produces faster recovery. |
DOES THIS APPLY TO YOU? If fatigue is present but breathlessness on exertion is not, and the tiredness is persistent and unresponsive to sleep, low iron is a likely contributor but thyroid function and cortisol patterns are also worth considering. If breathlessness is present at rest rather than only on exertion, see a GP before attributing it to iron alone. |
Hair follicles are among the fastest-dividing cells in the body. Fast cell division requires substantial oxygen and therefore substantial iron-dependent haemoglobin delivery. When iron is depleted, the body deprioritises blood flow to hair follicles, which are non-essential for survival, to preserve oxygen delivery to critical organs.
The hair follicle responds to this reduced blood supply by shifting from the growth phase (anagen) into the resting phase (telogen) prematurely. After the resting phase, the hair falls out. This is called telogen effluvium and it is one of the most consistent findings in iron deficiency. The hair loss typically presents as diffuse thinning across the scalp rather than patches, with increased shedding visible in the shower, on pillows, and in hairbrushes.
The timeline matters. Hair follicle changes take two to three months to produce visible shedding, which means the iron depletion that caused the hair loss may have started three to four months before the hair loss became obvious. Many people are surprised when a blood test confirms low iron because the hair loss feels recent, but the deficit that caused it is not.
WHAT TO DO ABOUT IT Hair loss from iron deficiency requires iron restoration to resolve. Topical treatments and hair supplements do not address the oxygen deficit at the follicle. Restoring serum ferritin is the relevant target. Hair regrowth from ferritin restoration is typically noticeable at three to six months, reflecting the three to four month hair growth cycle. This is not a fast fix. The shedding reducing is the first sign of improvement. Regrowth visible at the scalp comes later. |
DOES THIS APPLY TO YOU? If hair loss is specifically diffuse thinning rather than patches, and coincides with other low iron symptoms or a period of high demand, heavy periods, or low dietary iron, the iron mechanism is the most likely driver. Patchy hair loss, sudden onset, or hair loss with scalp changes suggests different mechanisms that warrant dermatological assessment. |
Temperature regulation depends on peripheral blood flow. Warm blood from the core reaches the hands and feet and keeps them at a comfortable temperature. When iron is low and oxygen delivery per unit of blood is reduced, the body constricts peripheral blood vessels to divert more blood to core organs. The extremities receive less blood flow and become cold.
This is not a circulation problem in the cardiovascular sense. The heart is functioning. The blood vessels are responding normally to a signal from the body to preserve oxygen delivery to essential organs. The cold hands and feet are a consequence of the body correctly prioritising its resources in conditions of oxygen scarcity. Restoring iron restores oxygen delivery and peripheral circulation returns to normal.
The cold often extends to a generalised feeling of being cold in conditions where others are comfortable. This reflects the broader thermal regulation deficit rather than just extremity blood flow.
DOES THIS APPLY TO YOU? If cold extremities are present alongside the other low iron symptoms, particularly fatigue and pale inner eyelids, iron is a likely driver. If cold hands and feet are present in isolation without other iron symptoms, Raynaud’s phenomenon, thyroid dysfunction, or other circulatory factors are more likely mechanisms and warrant different assessment. |
Restless legs syndrome, the uncomfortable urge to move the legs at rest that is typically worse at night and relieved by movement, has a well-documented association with iron deficiency. The mechanism is specific.
Iron is required for the production of dopamine in the brain. Dopamine governs movement control, including the inhibitory signals that keep legs still at rest. When iron is depleted, dopamine production is impaired and the inhibitory signal weakens. The legs receive a movement urge signal without adequate dopamine to quieten it. This is why the restlessness is specifically at rest and relieved by movement: movement generates its own sensory input that overrides the signal temporarily.
Restless legs from iron deficiency is distinct from restless legs with other causes. The iron connection is most likely when restless legs develop alongside other iron symptoms and particularly in contexts of known blood loss such as heavy periods or pregnancy.
WHAT TO DO ABOUT IT Restless legs from iron deficiency responds to iron restoration. The timeline for improvement is typically four to eight weeks of addressing the iron deficit. If restless legs are severe and significantly disrupting sleep, GP assessment is appropriate, as pharmaceutical interventions may be indicated alongside iron restoration. Magnesium deficiency can compound restless legs independently of iron, and addressing both simultaneously often produces better results than addressing either alone. |
The connection between restless legs, mineral deficiency, and sleep disruption is covered in our post on magnesium deficiency symptoms and why the mineral overlap matters.
Brain fog from low iron follows the same mechanism as fatigue: the brain is an extremely oxygen-intensive organ, consuming approximately 20 percent of the body’s total oxygen supply despite being only two percent of body weight. When oxygen delivery falls, cognitive processing slows. Thinking becomes effortful. Concentration and memory suffer. This is often one of the most distressing symptoms for people because it affects work and daily function in ways that tiredness alone does not.
Heart palpitations occur because the heart compensates for reduced oxygen per unit of blood by beating faster to circulate more blood. Most people experience this as an awareness of their heartbeat, occasional racing, or fluttering, particularly during light physical activity. In the absence of a heart condition, palpitations that coincide with other low iron symptoms almost always resolve as iron is restored.
Headaches from low iron result from reduced oxygen delivery to the brain producing vasodilation, the widening of blood vessels in an attempt to deliver more oxygenated blood. The vasodilation itself produces the headache sensation.
Pale skin and pale inner eyelids are a direct consequence of reduced haemoglobin. Haemoglobin is what gives blood its red colour. Less haemoglobin means less colour in the blood and therefore in the skin and mucous membranes. The inside of the lower eyelid is a reliable indicator: if it is pale pink or white rather than deep red, haemoglobin is likely low.
DOES THIS APPLY TO YOU? Brain fog and palpitations present in a cluster alongside fatigue, cold extremities, and hair thinning strongly indicates low iron or iron deficiency anaemia. Either symptom in isolation without the cluster warrants broader assessment including thyroid, cortisol, and cardiovascular evaluation before attributing it to iron alone. |
This is the section that explains why many people with clear iron deficiency symptoms are told their blood results are normal.
A standard blood count measures haemoglobin. The body protects haemoglobin levels by drawing on stored iron, measured as ferritin. You can have low ferritin, meaning your iron stores are depleted, and still have haemoglobin in the low-normal range. Your doctor sees a normal haemoglobin and tells you your iron is fine. But your ferritin is telling a different story.
Ferritin is the more sensitive marker for functional iron status. Symptoms of iron deficiency, including fatigue, hair loss, restless legs, and brain fog, typically appear when ferritin is low even if haemoglobin has not yet fallen below the clinical anaemia threshold. This is the pre-anaemic state and it is where most people with symptomatic iron deficiency actually sit.
If you have had a blood test and been told your iron is normal, ask specifically whether ferritin was measured and what the value was. A ferritin below 30 micrograms per litre is associated with symptoms in many people, even though some laboratories use reference ranges with a lower limit of 12 or 15. Optimal ferritin for symptom resolution is generally considered to be above 50 micrograms per litre in adults, and higher still for those with significant hair lo
DEFINITION FERRITIN A protein that stores iron in cells, primarily in the liver, spleen, and bone marrow. Ferritin is the body’s iron reserve. When dietary iron intake or absorption is insufficient, ferritin falls first, before haemoglobin. Symptoms of iron deficiency often appear when ferritin is low even if haemoglobin remains within the reference range. This is called iron deficiency without anaemia or pre-anaemia. A standard full blood count does not always include ferritin. It needs to be specifically requested. Ferritin is the more diagnostically sensitive marker for functional iron status. |
WHAT TO DO ABOUT IT If your symptoms fit and your standard blood test was normal, specifically request ferritin alongside a full blood count at your next GP appointment. A ferritin result in the lower end of the reference range, even technically within range, combined with symptoms, is sufficient clinical reason to trial iron restoration. Discuss with your GP whether dietary iron increases or supplemental iron is the appropriate approach for your situation. |
Iron deficiency is significantly more common in women than men for one primary reason: menstruation. Each menstrual cycle involves blood loss ranging from approximately 30 to 80 millilitres in a typical cycle and up to 200 millilitres or more in heavy periods. Each millilitre of blood lost contains approximately 0.5 milligrams of iron. A heavy period can represent a monthly iron loss that the diet alone may not fully replace.
This creates a cumulative deficit that builds over months and years. The symptoms arrive gradually and are often attributed to stress, poor sleep, or working too hard. The connection to iron is missed because the fatigue and hair thinning did not appear immediately after a period but accumulated over time.
Pregnancy compounds the risk significantly. The body requires substantially more iron during pregnancy to support the developing foetus and the expanded blood volume. Women who enter pregnancy with borderline ferritin are at high risk of symptomatic iron deficiency during the second and third trimesters when iron demand peaks.
The perimenopause and post-menopause transition creates a different pattern. Heavy or irregular periods in perimenopause can accelerate iron depletion, while post-menopause women without significant blood loss often see iron status improve. Women in their thirties and forties experiencing heavy periods alongside fatigue, hair loss, and cold intolerance should always have ferritin measured as part of the assessment.
DOES THIS APPLY TO YOU? If you are premenopausal with heavy periods and experiencing the symptom cluster described in this post, iron is the most likely primary driver and ferritin is the most important test to request. If symptoms are present but periods are normal or light, iron is still possible but thyroid dysfunction, particularly hypothyroidism, produces an almost identical symptom cluster and should be tested simultaneously. |
The hormonal picture that connects heavy periods, low progesterone, and iron depletion is covered in our post on low progesterone symptoms and the hormonal mechanism behind cycle-related depletion.
The approach depends on the severity of the deficit and its cause. Here is the honest hierarchy.
Request a full blood count with ferritin and transferrin saturation from your GP. Do not rely on haemoglobin alone. Ask for the ferritin number, not just whether it is normal. Know what your baseline is before supplementing.
Dietary iron comes in two forms. Haem iron from red meat, liver, and seafood is the most bioavailable form, absorbing at 15 to 35 percent. Non-haem iron from plant sources absorbs at two to five percent. Vitamin C significantly increases non-haem iron absorption when consumed at the same meal. Tea, coffee, and calcium significantly reduce it.
For people with moderate deficiency, dietary changes combined with supplementation produce the fastest results. For severe deficiency or clinical anaemia, GP-prescribed iron supplementation or intravenous iron may be required.
Iron works alongside other minerals. Zinc and magnesium are depleted by the same patterns of high demand and poor dietary diversity that deplete iron. Low zinc impairs immune function and testosterone signalling. Low magnesium impairs GABA function, energy production, and sleep quality. People with iron deficiency often have concurrent zinc and magnesium depletion, and addressing all three produces better recovery than addressing iron alone.
Shilajit resin delivers zinc, magnesium, and over 80 trace minerals alongside fulvic acid, which supports mineral absorption. It is not a substitute for iron supplementation when iron is clinically low. It may support the broader mineral balance that accompanies iron deficiency recovery. This is one option among others: dietary zinc from meat and seeds and dietary magnesium from nuts and legumes are the dietary foundation for addressing co-depletion.
Why ionic mineral delivery matters for cellular function is covered in our post on mineral bioavailability and why the form of a supplement determines whether it reaches your cells.
WHAT TO DO ABOUT IT Step one: test ferritin specifically, not just haemoglobin. Step two: if ferritin is below 50, increase haem iron intake through diet and discuss supplementation with your GP. Step three: address concurrent mineral deficiency in zinc and magnesium alongside iron, as they are frequently co-depleted and the body’s recovery is faster when all three are restored. Step four: retest ferritin at twelve weeks to confirm the deficit is closing. |
Fatigue, hair loss, cold intolerance, and cognitive slowing are produced by several different mechanisms. Iron deficiency is one. Thyroid dysfunction, particularly hypothyroidism, produces an almost identical symptom cluster and is more common in women. Magnesium deficiency produces fatigue, cold sensitivity, and sleep disruption through a different mechanism. Cortisol dysregulation from chronic stress produces fatigue and brain fog through HPA axis depletion rather than oxygen delivery failure.
The distinguishing features of the iron pattern: hair loss is specifically diffuse scalp shedding rather than patchy loss; restless legs at night are a consistent accompanying feature; pale inner eyelids are a visible indicator; breathlessness on light exertion is present. These four features together point more specifically toward iron than toward thyroid or magnesium.
The distinguishing features of hypothyroidism: weight gain rather than weight stability; cold intolerance that is generalised rather than peripheral; constipation; dry skin; and the fatigue tends to be heavier and more constant rather than effort-dependent. A TSH blood test distinguishes the two definitively.
The distinguishing feature of magnesium deficiency: muscle cramps and twitching are more prominent; sleep disruption is more specifically about settling rather than restless legs; anxiety is a more consistent feature. The two often occur together.
If you are unsure which pattern applies, request a full blood count with ferritin, TSH, and serum magnesium from your GP. These three tests together cover the most common causes of this symptom cluster.
Standard Thinking | The Biological Reality |
|---|---|
If my blood test was normal, my iron is fine | Standard blood tests measure haemoglobin. Ferritin, the stored iron measure, is a separate and more sensitive test that needs to be specifically requested. Symptoms of iron deficiency frequently appear when ferritin is low even if haemoglobin is within the normal range |
Iron deficiency just makes you tired | Iron deficiency reduces oxygen delivery to every tissue simultaneously. Fatigue is the most common symptom but hair loss, cold extremities, restless legs, brain fog, palpitations, and headaches all trace to the same cellular oxygen deficit |
Hair loss from low iron will stop once I start supplements | Hair follicle changes take two to three months to produce visible shedding. Recovery after ferritin restoration takes another three to six months to become visible. The fix works but the timeline is the full hair growth cycle, not weeks |
Restless legs is a separate sleep problem unrelated to iron | Restless legs has a well-documented association with iron deficiency through the dopamine production mechanism. In people with concurrent iron symptoms, iron restoration is the first intervention to trial before other treatments |
What are the main symptoms of low iron?
The core low iron symptom cluster includes persistent fatigue that does not fully resolve with rest, hair thinning and increased shedding, cold hands and feet, restless legs particularly at night, pale skin and pale inner eyelids, brain fog and difficulty concentrating, heart palpitations during light exertion, shortness of breath on activity that previously caused none, brittle nails, and persistent headaches. These symptoms all trace to the same mechanism: insufficient haemoglobin delivering oxygen to cells. The number and severity of symptoms generally reflects the depth of the iron deficit.
Can you have low iron symptoms with a normal blood test?
Yes. Standard blood tests measure haemoglobin. The body protects haemoglobin levels by drawing on stored iron, measured as ferritin. Ferritin can be significantly depleted while haemoglobin remains within the normal range. Symptoms of iron deficiency, including fatigue, hair loss, and restless legs, typically appear when ferritin falls even if haemoglobin has not yet fallen below the clinical anaemia threshold. If your standard blood test was normal but symptoms persist, ask your GP specifically for ferritin to be measured. A ferritin below 30 to 50 micrograms per litre in a symptomatic person is clinically significant regardless of whether it falls within the laboratory reference range.
Why does low iron cause hair loss?
Hair follicles are fast-dividing cells that require substantial oxygen delivery. When iron is low and haemoglobin is reduced, the body deprioritises blood flow to hair follicles in favour of essential organs. The follicles respond by shifting prematurely from the growth phase into the resting phase, after which the hair falls out. This process, called telogen effluvium, produces diffuse thinning across the scalp rather than patches. The hair loss typically becomes visible two to three months after the iron depletion began, and recovery takes three to six months of restored ferritin to produce visible regrowth.
Does low iron cause restless legs?
Yes, through the dopamine mechanism. Iron is required for dopamine production in the brain. Dopamine governs movement control, including the inhibitory signals that keep legs still at rest. When iron is depleted, dopamine production falls and the inhibitory signal weakens, producing the uncomfortable movement urge characteristic of restless legs syndrome. The connection is strongest when restless legs develop alongside other iron symptoms or in the context of known iron losses such as heavy periods or pregnancy. Iron restoration typically improves restless legs over four to eight weeks.
How long does it take to recover from iron deficiency?
The timeline depends on the severity of the deficit and whether the underlying cause has been addressed. Energy levels typically begin improving within two to four weeks of adequate iron restoration. Restless legs improve over four to eight weeks. Hair shedding reduces within six to eight weeks, but visible regrowth takes three to six months due to the hair growth cycle. Ferritin levels take three to six months to restore from significant depletion with consistent supplementation. The full resolution of all symptoms requires ferritin to reach an optimal level, generally above 50 micrograms per litre, and to remain there consistently.
ONE MORE THING BEFORE YOU GO If your symptom pattern does not quite match what is described here, tell us in the comments. Tell us the three symptoms that have been most persistent and how long they have been present. We read every comment and respond with what the research says about your specific picture. If you have already had your iron tested and it came back normal but symptoms persist, that is a specific and important question. Mention it and we will address it directly. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are on medications that affect electrolyte levels or are experiencing significant symptoms, consult a qualified healthcare provider before self-managing potassium intake.
Never Miss any Updates From Blog!




No products in the cart.