Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
Something is shifting. Your periods have changed. You are waking at 3am drenched in sweat. Your mood swings arrive without warning. You are exhausted in a way that sleep is not fixing.
These are not random. They are predictable biological responses to a specific hormonal transition, and each one has a mechanism that explains it.
Perimenopause is not a disease and it is not a deficiency. It is the transition phase before menopause, typically lasting four to ten years. The symptoms people struggle with most come from how oestrogen and progesterone behave during this transition: not a smooth decline but an unpredictable pattern that can feel more disruptive than menopause itself.
This post explains what is actually happening hormonally, why each major symptom category occurs, and what the evidence says about managing perimenopause and finding relief from its most disruptive symptoms.
BEFORE YOU READ FURTHER This post covers the hormonal mechanisms behind perimenopause symptoms and what research indicates may help. It addresses the most common symptom categories including vasomotor symptoms, menstrual changes, sleep disruption, mood changes, and physical symptoms. If you are experiencing symptoms that significantly affect your quality of life, if you have unusual or heavy bleeding, if symptoms appeared before age 40, or if you are unsure whether what you are experiencing is perimenopause or another condition, please see a GP. Hormone Replacement Therapy (HRT) is the clinically established treatment for significant perimenopausal symptoms and your GP is the appropriate first contact. This post is educational, not a substitute for clinical assessment. The mechanisms described here are relevant for women in their late 30s through early 50s who are noticing changes in their cycle, sleep, mood, or physical symptoms and want to understand what is driving them. If that is your situation, read on. |
DEFINITION PERIMENOPAUSE The transitional phase preceding menopause during which the ovaries gradually reduce their production of oestrogen and progesterone. It typically begins in the mid-to-late 40s, though onset from the mid-30s is not uncommon. Perimenopause ends twelve months after the final menstrual period, at which point menopause is confirmed. The duration is typically four to ten years. Unlike menopause itself, perimenopause is characterised by hormonal fluctuation rather than simple decline: oestrogen levels can spike high and crash low unpredictably before the overall trend downward, which is why symptoms are often more disruptive during perimenopause than after menopause has been confirmed. |
Before the mechanism, a quick check. Mark how many of these have been present for you consistently over the past three to six months.
Your periods have changed. They may be heavier, lighter, longer, shorter, or arriving at irregular intervals. The predictability you had is gone.
You are waking in the night with heat or sweating that is not explained by the room temperature. This may be accompanied by a racing heart or feeling of anxiety on waking.
Your mood feels less stable than your baseline. Irritability, sudden low mood, or anxiety that arrives without obvious external cause.
Your sleep quality has changed independently of hot flushes. Difficulty falling asleep, staying asleep, or waking too early and not returning to sleep.
You notice brain fog, word-finding difficulty, or slower processing that is new and not explained by sleep deprivation alone.
Your body feels different. Joint aches, skin changes, bloating, headaches, or fatigue that does not respond to rest the way it used to.
Your sex drive has changed, or you notice vaginal dryness or discomfort during sex that was not previously present.
If four or more of these apply and you are in your late 30s to early 50s, the perimenopause mechanism described below is the most likely explanation. The section below explains what is actually happening hormonally.
Most women enter perimenopause in their mid-to-late 40s. The average age of menopause in Australia is 51, meaning perimenopause typically spans the four to ten years before that. Onset from the mid-to-late 30s is within the normal range.
However, onset from the mid-30s is more common than most people realise. Perimenopause beginning at 35, 36, or 37 is within the normal range. The term ‘premature ovarian insufficiency’ applies to onset before age 40. If you are experiencing these symptoms in your mid-to-late 30s and your GP has not raised perimenopause as a possibility, it is worth raising it yourself.
The age at which your mother went through menopause is a reasonable predictor of when you will. Smoking is associated with earlier onset. Stress load, as described below, can influence the severity of symptoms at any age.
Fertility during perimenopause: irregular periods do not mean you cannot conceive. Ovulation still occurs, just less predictably. Effective contraception remains necessary until twelve months after the final period if pregnancy is not desired.
DOES THIS APPLY TO YOU? If your symptoms began before 40, if they appeared suddenly, or if you have a family history of early menopause, premature ovarian insufficiency should be ruled out by your GP before assuming a typical perimenopause timeline. The management approach differs significantly from typical perimenopause. |
Understanding when perimenopause begins matters less than understanding what is actually driving the symptoms. The hormonal mechanism is the same regardless of age.
Perimenopause is a clinical diagnosis based on symptoms, age, and cycle changes. There is no single blood test that confirms it, because hormone levels fluctuate too significantly during this phase for a single reading to be reliable.
Hormone levels, particularly FSH (follicle-stimulating hormone) and oestrogen, fluctuate significantly during perimenopause. A single reading can be misleading: oestrogen can be high one week and low the next. A normal FSH level does not rule out perimenopause and an elevated FSH does not definitively confirm it. This is why clinical guidance from the British Menopause Society and similar bodies recommends diagnosis based on symptom pattern and age rather than on blood tests alone in women over 45.
What actually confirms perimenopause: the combination of your age, your symptom pattern, changes to your cycle, and the absence of other explanations for your symptoms. Your GP may order blood tests to rule out other conditions such as thyroid dysfunction or iron deficiency, both of which produce overlapping symptoms, but those tests are to exclude alternatives rather than to confirm perimenopause itself.
Perimenopause versus thyroid dysfunction versus iron deficiency: these three conditions share fatigue, brain fog, and mood changes. The following patterns are worth raising with your GP rather than using as self-diagnostic criteria. Thyroid dysfunction often presents with weight change without dietary explanation, cold intolerance, and constipation. Iron deficiency often presents with breathlessness on exertion, pale inner eyelids, and restless legs. Perimenopause is more likely when symptoms track with menstrual cycle changes and when vasomotor symptoms are part of the picture. A thyroid panel and iron studies are simple to arrange and your GP should run both if there is any uncertainty.
DOES THIS APPLY TO YOU? If you are in your 40s and recognise the perimenopause pattern described in this post, you do not need a blood test before seeking GP support. You can present your symptom history and ask for a perimenopause assessment. If you are under 40, or if your GP is uncertain, blood tests can provide useful supporting information. The diagnosis does not depend on a positive result. |
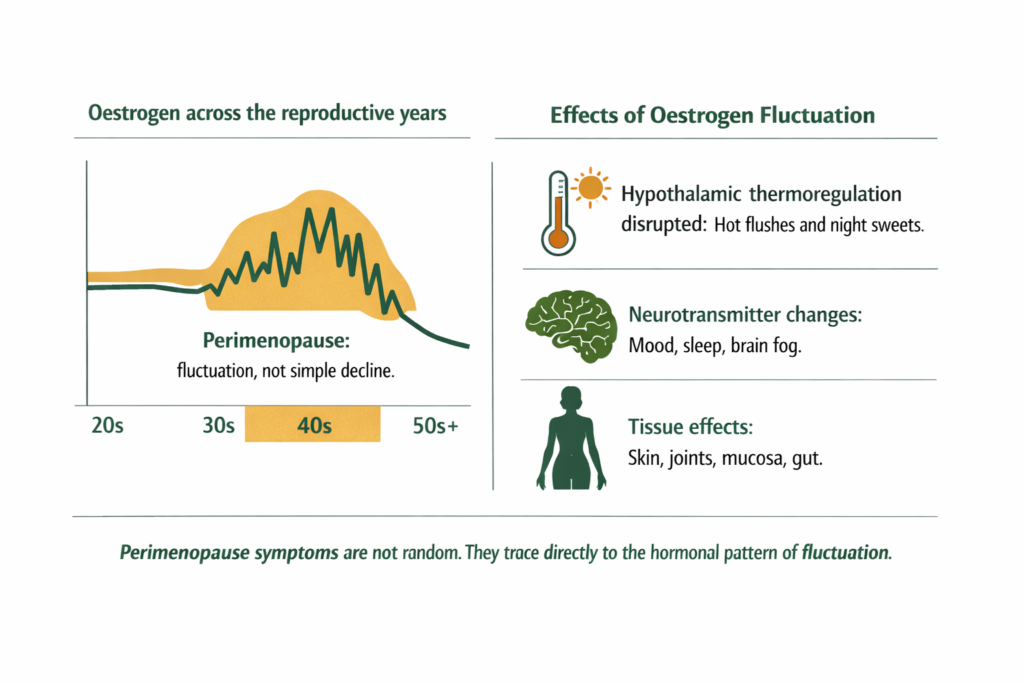
The most important thing to understand about perimenopause is that oestrogen does not follow a straight downward line. Levels can spike higher than in the reproductive years and crash low again, sometimes within the same week. This hormonal instability, not just the overall trend, is what drives many of the most disruptive symptoms.
Progesterone declines earlier and more steadily than oestrogen, beginning to fall as ovulation becomes less regular. Since progesterone is produced primarily after ovulation, fewer ovulatory cycles means less progesterone. This relative progesterone deficit in the context of still-fluctuating oestrogen is associated with the heavy periods, breast tenderness, bloating, and mood changes that are common in early perimenopause.
As perimenopause progresses, oestrogen levels trend downward on average even while continuing to fluctuate. The hypothalamus, which uses oestrogen signalling to regulate body temperature, becomes sensitive to these fluctuations. Small drops in oestrogen can trigger vasomotor responses: the hot flush and night sweat are the body’s thermoregulatory system responding to what it interprets as a temperature signal.
Oestrogen also influences serotonin, dopamine, and GABA pathways. When levels fluctuate sharply, mood regulation becomes less stable, sleep architecture is disrupted, and the cognitive functions that rely on these neurotransmitters, including memory and word retrieval, can be temporarily impaired.
DEFINITION VASOMOTOR SYMPTOMS The medical term for hot flushes and night sweats in perimenopause. They are caused by oestrogen fluctuation affecting the hypothalamus, the brain region that governs body temperature regulation. The hypothalamus misinterprets the hormonal shift as a rise in core body temperature and triggers heat-dissipation responses: blood vessel dilation, sweating, and a sensation of intense heat. They can last from seconds to several minutes and may be accompanied by heart palpitations or anxiety. Vasomotor symptoms affect around 75 percent of perimenopausal women. HRT is the most clinically established intervention for significant vasomotor symptoms. |
WHAT TO DO ABOUT IT If vasomotor symptoms are significantly disrupting your sleep or daily function, a GP conversation is the appropriate first step. HRT is the most evidence-based option for significant vasomotor symptoms and is appropriate for most women without specific contraindications. If symptoms are mild to moderate, the supportive measures described later in this post may be worth exploring alongside monitoring. These are not replacements for clinical care where that is indicated. |
DOES THIS APPLY TO YOU? If hot flushes and night sweats are manageable and not disrupting your function significantly, the support measures described below may be sufficient. If they are waking you multiple times per night, affecting your concentration during the day, or producing anxiety or palpitations that feel alarming, please see your GP. HRT is safe for the majority of women and highly effective for vasomotor symptoms. The risk-benefit picture for HRT has improved significantly since earlier studies and your GP can explain the current evidence. |
Vasomotor symptoms are the most studied perimenopause symptom category. The others are less consistently addressed but no less real.
Changes to your period are usually the first perimenopause sign. They may appear years before hot flushes or other symptoms.
What changes and why: As ovulation becomes less regular, the hormonal signals governing the menstrual cycle become less predictable. Cycles may shorten (periods arriving every 21 days), lengthen (every 35 to 45 days), or become erratic. Flow may become heavier in early perimenopause as relative oestrogen dominance from declining progesterone stimulates more endometrial growth. It may become lighter and more sporadic as oestrogen itself declines. Cramping patterns may change. Spotting between periods is common.
All of these are normal expressions of the same underlying mechanism: the hypothalamic-pituitary-ovarian axis is recalibrating. The unpredictability is not a malfunction. It is the transition.
When to see a GP: irregular periods are expected in perimenopause. However, bleeding that is significantly heavier than your previous norm, periods lasting more than seven days, bleeding more frequently than every 21 days, bleeding after sex, or any bleeding after you have gone twelve months without a period warrants assessment. These can have other causes and ruling them out is appropriate.
DOES THIS APPLY TO YOU? If you have removed demand, rested, and done the physical stabilisation steps and you are not feeling any shift within 24 to 48 hours, or if symptoms are worsening rather than stabilising, please see a GP. A nervous breakdown that does not begin to stabilise with rest and reduced demand warrants clinical assessment to rule out conditions that require clinical management including severe depression, anxiety disorder, or other conditions that can present similarly. |
Menstrual changes are the body’s first signal that the reproductive transition has begun. The symptom categories below typically follow as oestrogen fluctuation becomes more pronounced.
Perimenopause disrupts sleep through two mechanisms that compound each other.
Night sweats wake the nervous system during sleep, fragment sleep architecture, and make returning to sleep difficult. This is the mechanism most people are aware of.
Progesterone’s role in sleep is less discussed but equally significant. Progesterone acts on GABA receptors, supporting the calming transition into deep sleep. As it declines, that effect diminishes. Many women wake around 3am feeling restless and activated, unable to return to sleep, even on nights without hot flushes.
Research also associates magnesium with GABA receptor activity and sleep quality. For the full sleep mechanism, see our post on why magnesium glycinate specifically supports sleep and what form actually works.
WHAT TO DO ABOUT IT Both mechanisms are worth addressing. For night sweat disruption, a cool bedroom and moisture-wicking bedding can reduce severity, and GP discussion of HRT is appropriate if symptoms significantly affect your sleep. For the progesterone-related GABA mechanism, magnesium in warm water before bed may offer some support through the same calming pathway. A small dose 30 to 60 minutes before sleep may be more relevant for this purpose than a morning-only approach. These are supportive considerations, not clinical instructions. |
Perimenopause mood changes are neurobiological, not psychological weakness.
Oestrogen influences serotonin and dopamine synthesis and receptor sensitivity. When levels shift sharply, these systems shift with them. The result is mood instability, increased anxiety, or emotional flatness arriving without clear external cause.
Brain fog includes word-finding difficulty, slower processing, and reduced working memory. Research suggests these cognitive symptoms track the hormonal instability phase and often improve once menopause is confirmed and hormone levels settle. They are not evidence of permanent cognitive decline.
Night anxiety or anxious waking is often linked to the cortisol response that follows a temperature shift after a hot flush, even a mild one that does not fully wake the sleeper.
High stress amplifies all of these symptoms. Women under sustained psychological stress consistently report more severe perimenopausal symptoms. Stress does not cause perimenopause, but elevated cortisol places additional demand on the systems already under pressure from hormonal change.
The GABA pathway behind sleep anxiety and mood is covered in full in our post on magnesium glycinate for anxiety and why the form determines whether it actually reaches the relevant receptors.
WHAT TO DO ABOUT IT If mood changes or anxiety are mild and linked to specific hormonal phases, the mineral and adaptogenic support layer described in the What Helps section below may be sufficient. If you are experiencing persistent depression that is affecting your ability to function, that warrants GP assessment regardless of whether perimenopause is the context. Perimenopause is a recognised risk period for depression and effective clinical treatment exists alongside the biological support approach. |
The physical symptom range of perimenopause is wide. This breadth surprises many people because the focus in mainstream discussion is almost entirely on periods and hot flushes. But oestrogen receptors are present throughout the body, and when oestrogen fluctuates, the tissues that depend on it respond.
Itchy skin and skin changes: Oestrogen supports collagen production and skin moisture. Fluctuating oestrogen can produce itching, dryness, and a change in skin texture. The itching often occurs on the arms, legs, or torso and is not associated with any rash or dermatological cause. It is an oestrogen-mediated skin response.
Joint and muscle pain: Oestrogen has anti-inflammatory properties. As levels fluctuate and decline, the joints lose some of this protection and may become more reactive, producing aching in the knees, hips, shoulders, or lower back that was not previously present. This is sometimes called musculoskeletal perimenopause syndrome and is one of the less discussed but commonly experienced symptom categories.
Fatigue: Perimenopause fatigue has multiple drivers. Disrupted sleep is one. Hormonal fluctuation requiring ongoing biological adaptation is another. The mineral depletion associated with elevated cortisol from the stress of managing an unpredictable body is a third. The fatigue is typically worse in the days before a period or during hormonal low phases.
Bloating, nausea, and digestive changes: Oestrogen influences gut motility and the gut microbiome. Fluctuating oestrogen levels are associated with digestive changes including bloating, nausea, heartburn, and looser stools. These tend to track with hormonal phases rather than being constant.
Dizziness and heart palpitations: Vasomotor changes affect blood vessel tone. Dizziness and palpitations that accompany hot flushes or occur independently are a recognised perimenopause expression. If palpitations are frequent, prolonged, or associated with chest pain or shortness of breath, cardiac causes should be ruled out by a GP.
DOES THIS APPLY TO YOU? Physical symptoms that are mild, intermittent, and accompanied by other recognisable perimenopause signs in the appropriate age range are almost certainly perimenopause. Physical symptoms that are severe, constant, or do not pattern with hormonal phases, or that include unexplained weight loss, persistent pain, or anything that feels alarming, warrant clinical assessment to rule out other causes first. |
The physical symptom range of perimenopause is broader than most people are told. Recognising these as hormonal responses rather than separate problems to investigate individually saves significant time and distress.
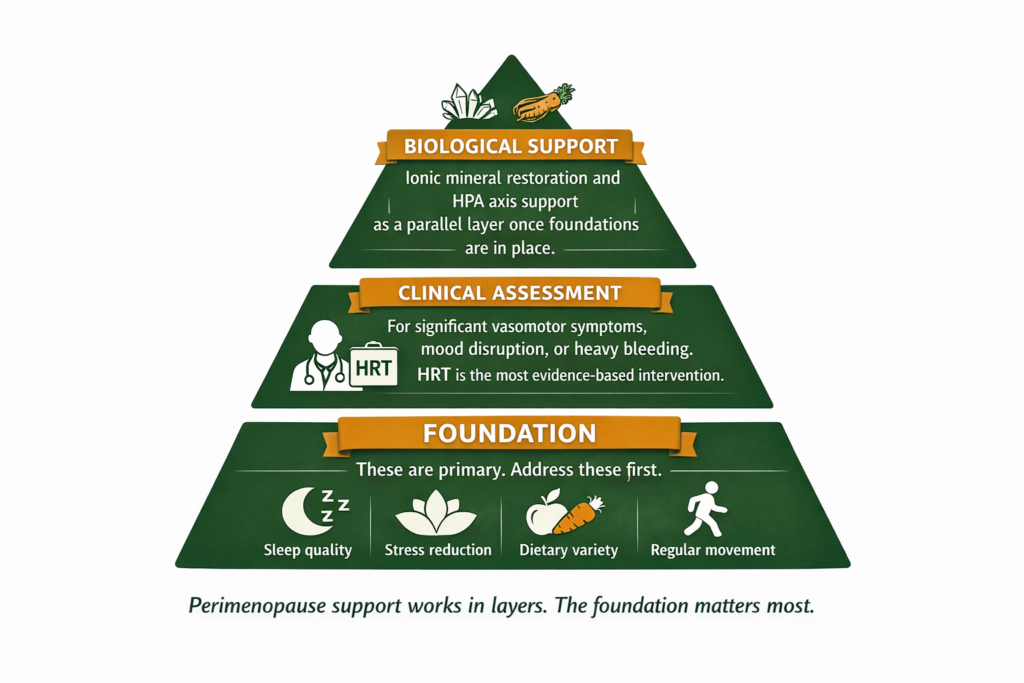
Before supplements or medications, the evidence is clearest for these foundations.
Sleep quality is the highest priority. Not just duration but architecture. The approaches in the sleep section above address this specifically. Poor sleep amplifies every other perimenopause symptom.
Stress load is the second priority. High cortisol from sustained psychological stress directly worsens perimenopause symptoms through the mineral depletion pathway and through the proposed hormonal competition mechanism described above. This is not generic wellness advice. It is a specific mechanism with a specific consequence. Reducing sustained cortisol demand during perimenopause is a genuine intervention.
Dietary patterns that support hormonal metabolism include adequate dietary protein, which provides amino acid precursors for neurotransmitter production, and reduced refined carbohydrate intake, which reduces the cortisol-spiking blood glucose fluctuations that compound hormonal instability. Phytoestrogens from whole soy, flaxseed, and legumes have a modest modulating effect on oestrogen activity, with the most consistent evidence in Asian populations with high habitual soy intake.
Regular moderate movement improves vasomotor symptom frequency and severity in research studies, supports mood through neurotransmitter pathways, and maintains bone density which begins to become a concern as oestrogen declines. High-intensity training that produces its own significant cortisol spike is less appropriate in this context than moderate, consistent activity.
HRT is the most clinically established intervention for perimenopause symptoms, particularly vasomotor symptoms, mood disruption, and sleep. The risk-benefit profile of HRT has been substantially reassessed since the Women’s Health Initiative study in 2002 and the current clinical consensus is that HRT initiated within ten years of menopause onset is appropriate for the majority of women without specific contraindications.
Your GP can assess your individual situation, discuss the current evidence, and help you determine whether HRT is appropriate and what type would best match your symptom profile. If your GP is not comfortable with this conversation, a specialist menopause clinic or gynaecologist with an interest in menopause is the appropriate next referral. Jean Hailes for Women’s Health (jeanhailes.org.au) and the Australasian Menopause Society (menopause.org.au) both provide evidence-based resources and clinician directories.
A note on HRT concerns: many women are hesitant about HRT because of concerns raised by the Women’s Health Initiative study published in 2002, which reported increased risks of breast cancer and cardiovascular disease. Subsequent analysis and multiple large studies have substantially revised this picture. Current clinical consensus from bodies including the British Menopause Society and the International Menopause Society indicates that for most healthy women under 60 or within ten years of menopause, the benefits of HRT outweigh the risks. The type, dose, and form of HRT significantly affect the risk profile. Your GP can explain the current evidence specific to your situation and medical history.
This post does not advise for or against HRT. That decision belongs with you and your GP, informed by your individual history and preferences.
Once the foundations are reasonably in place, a specific biological support layer addresses some of the mechanisms through which perimenopause symptoms are compounded.
Ionic magnesium supports the GABA receptor function that declining progesterone no longer supports as effectively. It contributes to the sleep-onset calming mechanism, supports the neurological stability that oestrogen fluctuation disrupts, and addresses the mineral depletion that elevated cortisol produces. Forms with higher bioavailability are generally preferred in research contexts on magnesium and hormonal symptoms.
Zinc supports immune function and hormonal enzyme pathways. It is involved in steroid hormone metabolism reactions and is particularly relevant for women experiencing hair changes, skin changes, or increased susceptibility to illness alongside hormonal symptoms.
Ashwagandha has RCT evidence for reducing perceived stress and cortisol in stressed adults (Chandrasekhar et al., 2012). It does not raise oestrogen or progesterone directly. Its relevance in perimenopause is as a stress amplifier reducer: high cortisol worsens hormonal fluctuation symptoms, and ashwagandha supports the HPA axis regulation that allows the stress response to settle more effectively.
The morning sipping protocol delivers ionic minerals continuously through the hours of highest cortisol activity: dissolve your daily portion of Shilajit resin and ashwagandha resin in one litre of warm water and sip from waking until approximately 2pm. For sleep support specifically, a small additional dose of ionic magnesium dissolved in warm water 30 to 60 minutes before bed addresses the GABA pathway through the evening rather than earlier in the day only. The full mechanism is covered in our post on what Shilajit resin delivers and why the ionic mineral form is the relevant variable.
WHAT TO DO ABOUT IT Start with the foundation layer first. Address sleep and stress load before adding any supplements. The biological support layer works most effectively when it is not fighting an ongoing cortisol demand that continues depleting what it is trying to restore. Once the foundation is reasonably managed, adding ionic mineral support and adaptogenic cortisol support in parallel with clinical assessment where appropriate gives you the most complete approach to the perimenopause transition. These tools support the biological environment during a real hormonal transition. They do not replace clinical care where that is indicated. |
DOES THIS APPLY TO YOU? If you have tried the foundation approaches and the biological support layer for eight to twelve weeks and are still significantly symptomatic, or if at any point your symptoms are affecting your ability to work, maintain relationships, or function in daily life, that is the appropriate point for GP assessment of HRT or other clinical support. The threshold for clinical intervention is not ‘cannot cope at all.’ It is ‘this is significantly affecting my quality of life.’ |
Standard Thinking | The Biological Reality |
|---|---|
Perimenopause is just your periods becoming irregular | Irregular periods are one early sign. The full perimenopause symptom range includes vasomotor symptoms, sleep disruption, mood changes, brain fog, joint pain, skin changes, fatigue, and digestive changes, all driven by the same hormonal fluctuation pattern |
Oestrogen just declines in perimenopause | Oestrogen fluctuates in perimenopause before the overall downward trend. It can spike to levels higher than in the reproductive years and crash low unpredictably. The instability of fluctuation, not just the direction of change, is what drives the most disruptive symptoms |
If symptoms are bad you just need to push through until menopause | Perimenopause lasts four to ten years. Waiting it out without support is not the only option. HRT is established as safe and effective for most women. Biological support for the compounding mechanisms is also available. Quality of life during this transition matters |
Supplements can replace HRT | Supplements address specific compounding mechanisms, particularly the cortisol load that worsens hormonal fluctuation symptoms and the mineral depletion that affects sleep and mood. They are not oestrogen and do not replace HRT where HRT is clinically indicated |
Brain fog and mood changes in perimenopause are psychological | They are neurobiological. Oestrogen fluctuation directly affects serotonin, dopamine, and GABA pathways. The cognitive and mood changes are physiologically driven. They are also often temporary: they tend to stabilise once menopause is confirmed and hormonal fluctuation settles |
The most common perimenopause symptoms fall into four categories. Vasomotor symptoms: hot flushes and night sweats, affecting around 75 percent of perimenopausal women. Menstrual changes: irregular cycles, heavier or lighter flow, new cramping patterns. Sleep disruption: difficulty falling asleep, staying asleep, or waking early, both from night sweats and from the decline in progesterone’s GABA-mediated sleep-promoting effect. Mood and cognitive changes: irritability, anxiety, low mood, brain fog, and word-finding difficulty driven by oestrogen’s influence on neurotransmitter systems. Physical symptoms including joint pain, itchy skin, fatigue, bloating, and digestive changes are less discussed but widely experienced. Any one of these categories can present first and at varying severity.
The average perimenopause onset is the mid-to-late 40s, with menopause itself typically occurring at around 51. However, onset from the mid-to-late 30s is within the normal range. Onset before age 40 is classified as premature ovarian insufficiency and warrants GP assessment as the management differs. Your mother’s menopause timing is a useful predictor of your own. Stress load and smoking are associated with earlier onset. If you are experiencing perimenopause symptoms in your late 30s and your GP has not raised perimenopause, it is worth raising it yourself.
Perimenopause typically lasts four to ten years, ending at the point of menopause, which is defined as twelve months after the final menstrual period. The most symptomatic period is often the final one to two years before menopause as hormonal fluctuation is at its most pronounced. Symptoms often improve once menopause is confirmed and oestrogen stabilises at a new lower baseline, though vasomotor symptoms can continue for several years after menopause for some women.
The evidence hierarchy runs from most to least established. HRT is the most evidence-based intervention for significant vasomotor symptoms, mood disruption, and sleep, and is appropriate for most women without specific contraindications. Lifestyle foundations including sleep quality, stress reduction, moderate regular movement, and dietary patterns that support hormonal metabolism have strong supporting evidence. Biological support addressing the compounding mechanisms, specifically the cortisol load that worsens hormonal fluctuation and the mineral depletion that affects sleep and mood, offers a supportive parallel layer. Any individual approach is most effective when the layers below it are reasonably addressed first.
Yes, through direct neurobiological mechanisms. Oestrogen influences serotonin, dopamine, and GABA pathways. When oestrogen fluctuates, these neurotransmitter systems fluctuate with it, producing mood instability, anxiety, and sometimes depression that has a recognisable hormonal quality: it arrives without a clear external cause, varies with hormonal phases, and may be accompanied by other perimenopause symptoms. Perimenopause is a recognised risk period for depression. If mood symptoms are mild to moderate and clearly hormonal in pattern, the biological support approach can help. If they are persistent, pervasive, or affecting function, GP assessment is appropriate. Perimenopause does not need to be endured without support.
|
ONE MORE THING BEFORE YOU GO If your perimenopause pattern does not match what is described here, or if you are trying to work out whether what you are experiencing is perimenopause or something else, leave it in the comments below. Tell us the three symptoms that feel most persistent, how long they have been present, and what you have already tried. We read every comment and respond with what the research says. If your symptoms are fitting the picture but you are not sure which layer to start with, that is specifically the kind of question we can help you work through directly. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Perimenopause symptoms overlap with a number of other conditions and individual presentations vary significantly. If you are experiencing symptoms that affect your quality of life or are concerned about any aspect of your health during this transition, consult a qualified healthcare provider. HRT decisions should be made in partnership with your GP based on your individual circumstances.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!




No products in the cart.