Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
Home Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body...
Read Article
You have tried everything. You go to bed at a reasonable hour. You avoid your phone. You have blackout curtains. Sometimes you fall asleep fine and then wake at 3am, completely alert, unable to get back down. Other nights you lie there for an hour, exhausted but wired, your mind running at full speed while your body just wants to stop.
You have probably tried magnesium. Maybe it helped a little. Maybe you noticed nothing and concluded it was not for you. If that is where you landed, that conclusion is almost certainly wrong. The magnesium did not fail you. The form of magnesium you took almost certainly did.
Our research indicates the single most overlooked variable in sleep supplementation is not the mineral itself. It is the form it arrives in, and whether your cells can actually use what the label claims is inside the capsule.
BEFORE YOU READ FURTHER If you have tried magnesium before and noticed nothing: this is not evidence that magnesium does not work for sleep. It is almost always evidence that the form you took did not deliver a meaningful dose to your cells. Magnesium oxide, the most common form in budget supplements and multivitamins, delivers approximately 4 percent of its stated dose to your cells. A 300mg capsule delivers roughly 12mg of usable magnesium. The explanation for why, and what to take instead, is the central argument of this post. See a healthcare provider rather than treating this as a magnesium issue if: your sleep disruption appeared suddenly alongside other new symptoms, you have a diagnosed sleep disorder such as sleep apnoea, you are taking medications that affect sleep or mineral absorption, or sleep disruption is severe enough to significantly affect your daily safety or function. The mechanism described in this post is most relevant for people experiencing a gradual, persistent pattern of poor sleep quality, difficulty staying asleep, or the 3am waking pattern, without a diagnosed underlying condition. |
Sleep is not a passive state. Your brain, nervous system, and muscles are running active maintenance processes throughout the night, and every one of those processes consumes minerals. By the time you wake, your body has spent eight hours drawing down its ionic mineral reserves without any dietary replenishment.
The sodium-potassium pump is the key mechanism here.
DEFINITION SODIUM-POTASSIUM PUMP A protein engine embedded in every cell membrane that pushes sodium ions out and pulls potassium ions in, thousands of times per second. This generates the electrical charge across the membrane that controls nerve signalling, muscle relaxation, and the transport of water into cells. It runs continuously including throughout sleep and requires a constant supply of ionic minerals, especially magnesium, to operate. When those reserves drop, the pump slows, and the electrical signals governing your nervous system and muscles become erratic. |
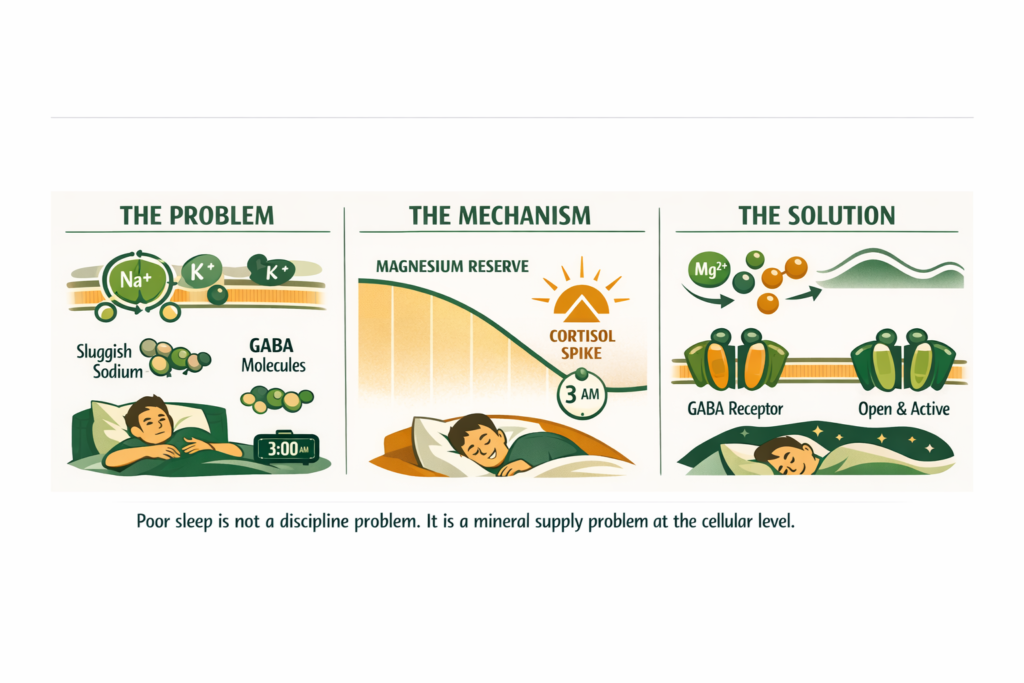
For sleep specifically, this pump governs two things that matter most. First, it regulates the electrical conditions required for GABA, your brain’s primary calming neurotransmitter, to work effectively. GABA is what allows your nervous system to downshift from the alert, activated state of daytime into the quieter state that sleep requires. Magnesium is a direct cofactor in GABA receptor function. Without adequate magnesium at the cell membrane level, GABA cannot do its job regardless of how tired you feel.
Second, the pump controls the electrical charge across muscle cell membranes. Muscle relaxation, the physical release that allows your body to stop being tense enough to sleep, depends on precise sodium-potassium ratios. When those ratios drift because the pump is running below capacity, muscles stay in a state of partial contraction. You feel it as restlessness, twitching, or the inability to physically settle even when your mind wants to.
We cover the full mechanism of how the sodium-potassium pump depletes and what restores it in our post on why drinking water may not be hydrating your cells.
The overnight mineral depletion cycle explains why so many people wake feeling unrefreshed despite hours in bed. The pump ran on depleted reserves all night. The maintenance processes were incomplete. The nervous system never fully downshifted. Sleep happened, but not the quality of sleep the biology was capable of producing.
WHAT TO DO ABOUT IT Restoring the ionic mineral supply the sodium-potassium pump requires changes what the overnight period produces. When the pump runs at capacity, GABA receptor function is maintained throughout the night. Muscle cell membranes hold their charge. The nervous system stays in the downshifted state. The maintenance processes complete. The result is not just falling asleep. It is staying asleep and waking with the sense that sleep actually did something. |
DOES THIS APPLY TO YOU? If you fall asleep without difficulty but wake during the night or wake unrefreshed, the depletion pattern during sleep is the most likely driver rather than the ability to fall asleep. If you struggle to fall asleep because you feel physically restless, muscle tension in the legs or body is the expression of the pump running below capacity before sleep begins. If your sleep problem appeared alongside a period of sustained stress lasting more than four to six weeks, the cortisol-mineral depletion pathway is almost certainly active and the GABA mechanism is compounded by that. |
But the depletion cycle is only half the story. There is a specific hour when it becomes critical and if you recognise this hour, the mechanism will make immediate sense.
If you wake at 3am regularly, this section is specifically for you.
The 3am waking pattern is not insomnia in the classical sense. It is a predictable biological event driven by two converging processes.
Process one: The body’s natural cortisol rhythm begins its morning rise at approximately 3am. In people whose stress regulation system is running properly, this rise is gradual and does not produce waking. In people with HPA axis dysregulation, the rise is sharper, more abrupt, and crosses the arousal threshold before it should. The person wakes feeling alert with a mild sense of unease they cannot explain.
DEFINITION HPA AXIS The hypothalamic-pituitary-adrenal axis is the three-part hormonal command chain governing the stress response. The hypothalamus detects a stressor and signals the pituitary, which signals the adrenal glands to release cortisol. When this system is dysregulated through chronic stress or mineral depletion, the cortisol rhythm loses its smooth pattern and begins producing sharp early-morning spikes that wake people at 3am. |
For a full explanation of HPA axis dysregulation and how adaptogens address it, read our post on what adaptogens actually do at the hormonal level.
Process two: After approximately five to six hours of sleep without mineral replenishment, magnesium reserves reach their lowest point of the 24-hour cycle. At this level, two things happen simultaneously. GABA receptor function weakens, reducing the nervous system’s ability to stay in a calm state. And the electrical threshold for neuronal firing drops, making the nervous system more reactive to the cortisol rise that is already beginning.
The two processes reinforce each other. The cortisol rise triggers arousal. The depleted magnesium means there is insufficient GABA support to buffer that arousal back into sleep. The person wakes and cannot return to sleep.
This also explains why 3am waking is so commonly accompanied by anxiety. Low magnesium directly increases neuronal excitability. The thoughts that arrive at 3am are not produced by a problem that did not exist at 10pm. They are produced by a nervous system running without adequate mineral support and therefore more reactive to the cortisol signal than it would be in a well-mineralised state.
WHAT TO DO ABOUT IT Raising the ionic mineral baseline before sleep raises the starting point from which the overnight depletion begins. A higher starting point means the depletion takes longer to reach the threshold that triggers the cortisol-GABA interaction at 3am. The morning sipping protocol addresses this directly: consistent ionic mineral delivery from waking until approximately 2pm ensures reserves are at their highest when the overnight decline begins. For the 3am waking pattern specifically, this is the intervention that addresses the cause rather than the symptom. |
DOES THIS APPLY TO YOU? If you wake specifically between 2am and 4am rather than at other times, and the waking comes with alertness or mild anxiety rather than a physical need, the cortisol-GABA mechanism describes your pattern precisely. If waking is at other times or for physical reasons such as needing the bathroom or pain, different mechanisms are more likely driving the disruption. If the 3am waking correlates with periods of higher stress at work or in life, the HPA axis dysregulation component is almost certainly active alongside the mineral depletion. |
Knowing why it happens tells you what direction the solution has to come from. But before the solution makes sense, you need to understand why the standard supplement most people reach for actively fails to address this.
The supplement industry is not deceiving you about magnesium. A bottle that states 300mg per capsule genuinely contains approximately 300mg. What the label does not tell you is that the form of magnesium inside determines how much of that 300mg your cells can actually receive and use.
Bioavailability is the term for this
DEFINITION BIOAVAILABILITY The percentage of any substance you consume that completes the full journey from ingestion through to active use inside your cells. A supplement can contain exactly what the label states and still deliver only a fraction of that dose biologically, depending entirely on its form. Two magnesium supplements can have identical label milligrams and produce entirely different outcomes at the cellular level. |
Here is what the research shows across the most common magnesium forms:
Form | Absorption Rate | From 300mg, Cells Receive | Commonly Found In |
|---|---|---|---|
Magnesium Oxide | 4% | ~12mg | Budget supplements, most multivitamins |
Magnesium Citrate | 25-30% | ~75-90mg | Mid-range supplements |
Magnesium Glycinate | 50-80% | ~150-240mg | Quality sleep supplements |
Ionic Magnesium | 85-95% | ~255-285mg | Natural mineral sources, Shilajit |
The person taking magnesium oxide is receiving approximately 12mg of usable magnesium from a 300mg capsule (Firoz and Graber, 2001). The sodium-potassium pump, the GABA system, and muscle cell electrical regulation all require meaningful magnesium levels to function. 12mg does not move that needle. This is not a failure of magnesium as sleep support. It is a failure of delivery.
Magnesium glycinate is the form with the strongest clinical evidence for sleep and anxiety outcomes. The mineral is bound to glycine, an amino acid that crosses into the nervous system and has its own calming properties. The chelated form absorbs at 50 to 80 percent, delivering 150 to 240mg of usable magnesium from a 300mg dose. That is the range at which the cellular mechanisms described above actually respond.
The complete breakdown of every mineral form and what each delivers to your cells is covered in our post on how mineral bioavailability determines what your supplement actually delivers.
WHAT TO DO ABOUT IT Check the label of any magnesium supplement you have tried. If it says magnesium oxide or is inside a multivitamin, you were absorbing approximately 4 percent of the stated dose. If it says magnesium citrate, you were in the 25 to 30 percent range. Both are meaningful improvements to move to glycinate or ionic forms before concluding magnesium does not work for your sleep. Switch the form before increasing the dose. |
DOES THIS APPLY TO YOU? If you tried magnesium glycinate consistently for four or more weeks at a meaningful dose and noticed limited sleep improvement, two variables remain to investigate before concluding the form is not relevant: dose and timing. Many glycinate supplements contain 100 to 150mg per capsule, which at 50 to 80 percent absorption delivers 50 to 120mg to cells. That is an improvement over oxide but may still be below the threshold for established depletion. And a single bedtime dose addresses the symptom window without addressing the overnight depletion baseline. The sipping protocol changes the starting point, not just the window. |
Understanding the form solves the ‘why it did not work before’ question. But the form is only one variable. When you deliver it, and how continuously, changes the outcome just as significantly.
Most guidance says to take magnesium 30 to 60 minutes before bed. This is not wrong, but it is not the most effective approach when understood against the mechanism.
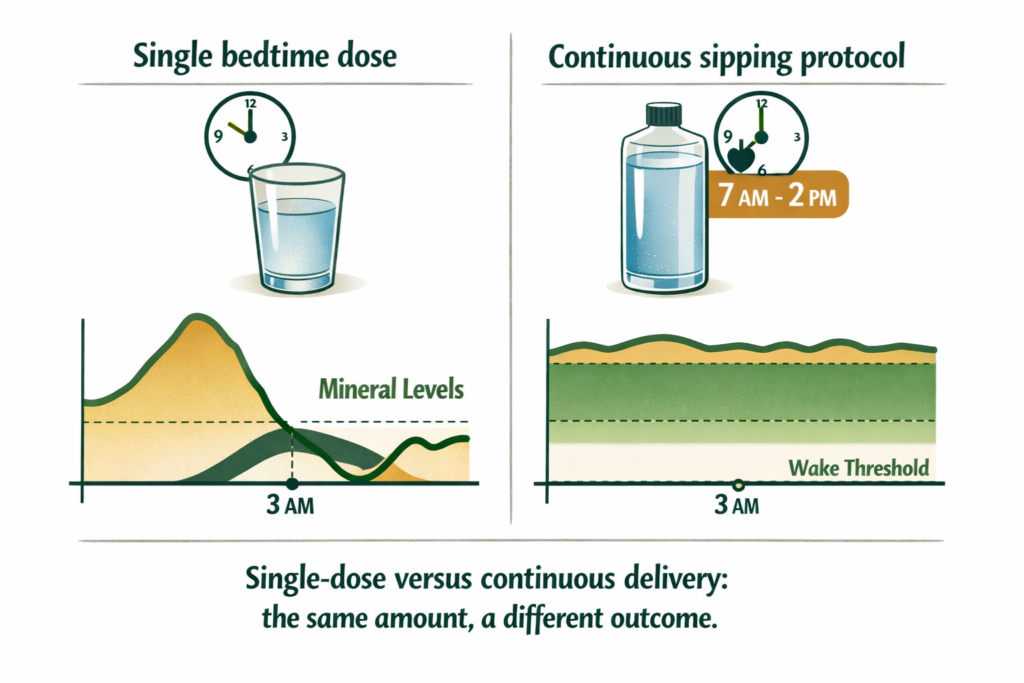
The sodium-potassium pump runs continuously throughout the day and night. By the time you take magnesium at 9pm, your cellular reserves have been declining since your last mineral intake. The overnight depletion cycle that produces the 3am wake begins from whatever level those reserves are at when you fall asleep. A higher starting point means a slower decline and a shallower or later cortisol spike.
The optimal protocol is dissolution in a one-litre bottle consumed steadily from waking until approximately 2pm. This keeps ionic mineral levels consistent through the hours of highest demand and ensures reserves are at their peak when the overnight decline begins. The afternoon cutoff is deliberate: Shilajit supports mitochondrial energy production and sustained intake past mid-afternoon can interfere with the natural wind-down the nervous system requires before sleep.
Taking a small additional dose 30 to 60 minutes before sleep remains useful, particularly for restless legs or muscle cramping at night. The sipping protocol addresses the root cause. The bedtime dose addresses the symptom.
WHAT TO DO ABOUT IT Start the morning sipping protocol immediately rather than waiting until bedtime to supplement. Dissolve the daily Shilajit portion in a one-litre bottle and sip from waking until approximately 2pm. Add a small additional dissolution in warm water 30 to 60 minutes before sleep if muscle cramping or restlessness at night is a specific symptom. Most people notice the first change in the restlessness and tension symptoms within three to five days. The 3am pattern typically responds within three to four weeks as reserves stabilise. |
DOES THIS APPLY TO YOU? If you have been taking magnesium at bedtime only and noticed some improvement in falling asleep but the 3am waking persists, the bedtime dose is working for the falling-asleep variable but not for the overnight depletion baseline. Switching to the sipping protocol while keeping the small bedtime dose specifically addresses the 3am pattern. If the sipping protocol produces afternoon energy that interferes with winding down at night, move the cutoff earlier, around noon, and observe whether sleep onset improves. |
Knowing the form and the timing leaves one more question: what does the most bioavailable form actually look like in practice, and how does it differ from what most people are buying?
Ionic minerals are minerals in their dissolved, electrically charged state. This is the form the sodium-potassium pump recognises directly. No digestive conversion required. No dependence on stomach acid levels or enzyme activity. The gut wall transports ionic minerals directly because it evolved doing exactly that: processing water that had traveled through mineral-rich geological formations, arriving pre-dissolved and pre-charged.
Naturally occurring Shilajit resin, formed over millennia through the compression and decomposition of mineral-rich organic matter in Himalayan rock formations, delivers magnesium and a full spectrum of trace minerals in this ionic state. Alongside the minerals, Shilajit contains fulvic acid, a small organic molecule that actively carries ionic minerals across the gut wall and through cell membranes.
DEFINITION FULVIC ACID A naturally occurring organic molecule formed through the geological decomposition of mineral-rich plant matter. Fulvic acid acts as a molecular transport carrier, actively escorting ionic minerals across the gut wall and through cell membranes. It is the delivery mechanism that distinguishes ionic mineral sources from standard mineral supplements. The human gut evolved alongside fulvic acid-rich water sources. It is not a novel supplement ingredient. It is a mechanism the body already knows how to use. |
This is not a claim that Shilajit is a sleep supplement. It is a description of what its delivery mechanism does: it restores the ionic mineral environment the sodium-potassium pump requires to run at full capacity through the night. When that pump runs properly, GABA works properly. When GABA works properly, the nervous system downshifts into sleep and stays there.
WHAT TO DO ABOUT IT The practical difference between glycinate and ionic delivery is not just the absorption percentage. It is also the spectrum. Glycinate delivers magnesium with high efficiency. Ionic Shilajit delivers magnesium alongside over 80 trace minerals in the same ionic state. The sodium-potassium pump requires a full electrolyte environment, not just magnesium in isolation. For people whose sleep problems are connected to the full overnight depletion pattern rather than magnesium alone, the full spectrum addresses the complete mechanism. |
DOES THIS APPLY TO YOU? If you have tried magnesium glycinate specifically at a meaningful dose for four or more weeks with the morning sipping protocol and sleep quality is still poor, a broader mineral deficit or the HPA axis dysregulation pathway is the more likely remaining variable. The cortisol post covers the adaptogenic support that addresses the HPA axis component alongside mineral restoration. If sleep apnoea has not been ruled out and you snore or have been told you stop breathing during sleep, that warrants clinical investigation before attributing persistent sleep disruption to mineral depletion. |
Realistic expectations matter. The mechanism is real but the timeline is not overnight.
First three to five days: Some people notice improved ability to physically relax before sleep. Muscle tension and restlessness are the fastest-responding symptoms because they depend directly on the pump’s moment-to-moment ionic mineral supply.
One to two weeks: GABA receptor function improves as cellular magnesium levels stabilise. The nervous system’s ability to downshift becomes more consistent. Time to fall asleep typically shortens.
Three to four weeks: If the 3am pattern was driven by mineral depletion, it should be noticeably reduced or resolved. Deep sleep quality improves as overnight maintenance processes have adequate mineral supply to complete.
What magnesium does not change: Magnesium does not address sleep problems driven primarily by sleep apnoea, pain, or environmental factors. If significant disruption persists after four weeks of proper ionic magnesium supplementation, a healthcare provider is the right next step.
Standard Thinking | The Biological Reality |
|---|---|
Take 300mg of magnesium for sleep | 300mg of magnesium oxide delivers 12mg to your cells. The number on the label is not the number that governs your sleep |
Magnesium helps you relax before bed | Magnesium governs GABA receptor function and sodium-potassium pump electrical regulation throughout the entire night, not just the 30 minutes before bed |
Take it 30 minutes before bed | A continuous morning sipping protocol builds the ionic mineral reserve that determines your starting point for overnight depletion. A bedtime dose alone addresses the symptom, not the cause |
I tried magnesium and it did not work | You almost certainly tried magnesium oxide or an insufficient dose. Glycinate and ionic forms produce measurably different cellular outcomes from identical stated milligrams |
Melatonin is the primary sleep supplement | Melatonin addresses the signal to sleep. Magnesium addresses the biochemical conditions required to stay asleep. They solve different parts of the problem |
A normal diet provides enough magnesium | Soil mineral depletion since 1950 has reduced food magnesium content by 40 to 80 percent. Dietary sources are no longer a reliable primary supply |
I have tried both magnesium glycinate and magnesium citrate and still have sleep problems. This suggests the form argument is overstated.
Two possibilities are worth separating. The first is insufficient dose. Many glycinate supplements contain 100 to 150mg per dose. At 50 to 80 percent absorption that delivers 50 to 120mg to cells, an improvement over oxide but still below the threshold at which GABA receptor and pump function respond meaningfully in people with established depletion.
The second is suboptimal timing. A single bedtime dose addresses the symptom window without addressing the overnight depletion cycle that begins from a depleted reserve. Switching to the morning sipping protocol frequently produces different results.
If both dose and timing have been optimised and sleep problems persist, there may be an additional variable: stress-driven HPA axis dysregulation requiring cortisol regulation alongside mineral restoration. That combination is addressed in our post on high cortisol symptoms and the mineral depletion cycle.
Magnesium glycinate helps with sleep through two complementary mechanisms. The magnesium component restores the ionic mineral supply required for GABA receptor function and sodium-potassium pump electrical regulation, both essential for the nervous system to downshift into sleep and stay there. The glycine component crosses into the nervous system independently and has its own calming effect on neuronal activity. Together they address sleep quality from two directions simultaneously. The glycinate form is used specifically because its 50 to 80 percent absorption rate delivers a meaningful dose where oxide at 4 percent does not.
The most effective approach is a morning to early afternoon sipping protocol that maintains consistent ionic mineral levels through the day, combined with a smaller dose 30 to 60 minutes before bed. The morning protocol ensures cellular reserves are at their highest when the overnight depletion cycle begins, which delays and shallows the mineral trough that typically triggers the 3am waking pattern. A bedtime dose alone addresses the symptom window without addressing the baseline depletion that produces the overnight pattern.
Muscle relaxation and physical restlessness are the fastest-responding symptoms, often noticeable within three to five days. GABA-mediated improvements in the ability to fall and stay asleep typically emerge over one to two weeks as cellular magnesium levels stabilise. Resolution of the 3am waking pattern, if driven by overnight mineral depletion, typically occurs within three to four weeks. The timeline reflects the time required to restore cellular reserves depleted over months or years, not just the time for a single dose to absorb.
For sleep outcomes specifically, glycinate outperforms citrate for two reasons. First, absorption rate: glycinate achieves 50 to 80 percent versus citrate at 25 to 30 percent, meaning glycinate delivers roughly twice the usable magnesium from the same stated dose. Second, the glycine component has direct nervous system calming properties that citrate does not. Citrate is a meaningful upgrade over oxide. Glycinate is a meaningful upgrade over citrate. Ionic magnesium delivers a further step beyond glycinate by eliminating the remaining absorption variables entirely.
The 3am waking pattern in most people without a diagnosed sleep disorder reflects the convergence of the body’s natural early cortisol rise with the overnight low point in ionic mineral reserves. When magnesium reserves are depleted, GABA receptor function weakens precisely as the cortisol signal begins rising, removing the buffer that would otherwise keep the person asleep through that transition. Restoring ionic magnesium levels through the sipping protocol raises the baseline from which the overnight depletion begins. Most people with this specific pattern see significant improvement within three to four weeks of consistent ionic magnesium supplementation.
ONE MORE THING BEFORE YOU GO If you read this post and something resonated but also left you with a question we did not fully answer, leave it in the comments below. We read every comment and respond with what the research says. We are not asking you to engage for the sake of it. We are offering to extend the conversation if something here pointed toward a question the post did not close. If a specific symptom, a specific product experience, or a specific part of the mechanism did not land clearly, tell us. That is genuinely useful for us to know and we will answer with the same standard of evidence this post was written to. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are experiencing persistent sleep disruption, consult a qualified healthcare provider.
Never Miss any Updates From Blog!




No products in the cart.