Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You sleep. You wake up tired. You get through the day on caffeine and willpower. By 3pm you are running on empty. You go to bed exhausted and do it all again tomorrow.
You have probably tried the obvious things. Sleeping more. Cutting out sugar. Exercise. Blood tests. Everything came back normal. Nothing fixed it.
The reason nothing worked is that you have been treating the symptoms, not the source. This post explains what is actually driving persistent fatigue and gives you a structured four-phase correction protocol based on the cellular mechanism most practitioners do not test for.
BEFORE YOU READ FURTHER This post covers the biological mechanisms behind persistent fatigue and a structured protocol for addressing them. Fatigue has many possible clinical causes including thyroid dysfunction, iron deficiency anaemia, sleep apnoea, and depression. If your fatigue is severe, appeared suddenly, is accompanied by unexplained weight loss, or has not improved despite adequate sleep and lifestyle changes over several months, please see your GP before attributing it to any single cause. If your blood tests have come back normal and you are still exhausted, the cellular mechanism described below is the most likely explanation that has not yet been addressed. |
Mark how many of these apply to you consistently.
DOES THIS APPLY TO YOU? If four or more of these apply and have been consistent for months rather than days, you are most likely dealing with a cellular energy deficit. This is distinct from lifestyle tiredness or burnout. It does not improve with more rest alone because the problem is energy production, not energy expenditure. The section below explains why. |
Before the mechanism, this section matters. Most people with persistent fatigue have already tried the obvious approaches. Here is why each one fell short.
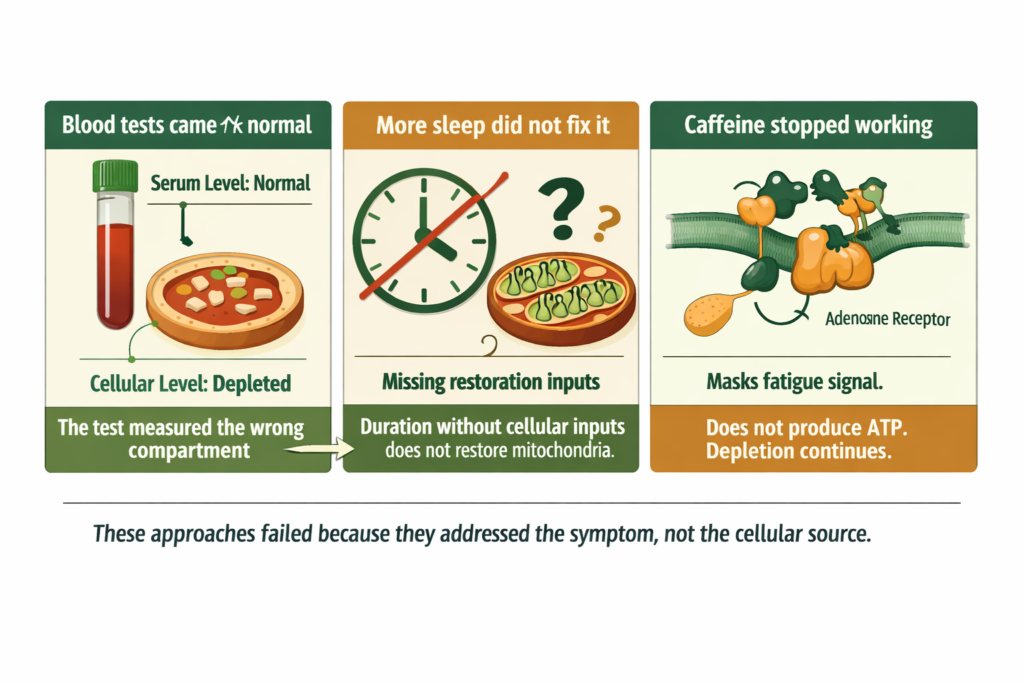
Standard blood tests measure mineral levels in the serum, the fluid surrounding your cells. The body maintains serum levels within a narrow range by pulling from bone, muscle, and tissue reserves when dietary intake is insufficient.
Your serum magnesium reads perfectly normal while your cells are operating on depleted reserves. The test measured the wrong compartment.
The number: Only 1 percent of total body magnesium is in the blood. A normal serum result does not confirm adequate cellular mineral status.
Because the problem is not sleep duration. It is what happens during sleep. Mitochondrial restoration and repair occur during the deepest sleep stages. If the raw materials required for that restoration are insufficient, you can sleep for nine hours and wake unrestored.
More time in bed does not solve a cellular input deficit. The inputs must be present for restoration to occur.
Caffeine does not produce energy. It blocks adenosine receptors that signal fatigue, masking the symptom without addressing ATP production.
The cellular depletion continues underneath the stimulation. Over time the body produces more adenosine receptors to compensate, requiring more caffeine to achieve the same masking effect. The underlying deficit compounds.
Once you understand why previous approaches failed, the solution becomes obvious. You were not failing at the approaches. The approaches were not addressing the mechanism.
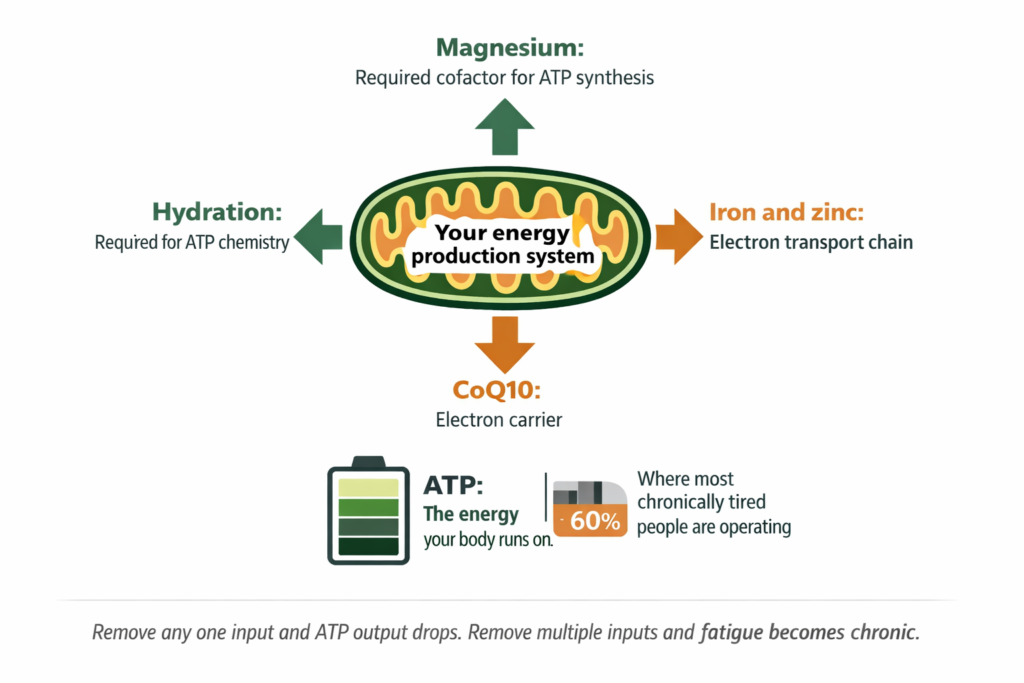
Your body runs on ATP, adenosine triphosphate. Every muscle contraction, every neurotransmitter release, every cellular repair process requires ATP. ATP is produced inside your mitochondria.
Mitochondrial output is not binary. It exists on a spectrum. Most people experiencing chronic low energy are not clinically ill. They are operating at 60 to 70 percent of their mitochondrial capacity and have normalised that as their baseline. They do not know what full energy feels like anymore.
Once clinical causes are excluded by a GP, this is the evidence-based order of priority for addressing persistent fatigue
Magnesium is required for ATP production. It is a cofactor for the enzymes involved in converting ADP back to ATP and for the electron transport chain reactions that generate the majority of cellular energy. Inadequate cellular magnesium directly reduces energy output. This is a biological dependency, not an association.
Iron is required for the electron transport chain. Zinc supports mitochondrial enzyme function. These are inputs the system cannot operate without, and they are not reliably reflected in standard serum tests.
Sustained high cortisol from psychological stress consumes cellular energy resources. Cortisol synthesis requires ATP. The sustained stress response draws from the same mitochondrial reserves that would otherwise power daily function.
High cortisol does not cause the primary cellular depletion but it dramatically amplifies it and accelerates the drain. People under sustained stress feel physically depleted even when they are not physically active.
Poor sleep is more often a consequence of cellular depletion and elevated cortisol than a root cause in its own right. Magnesium supports the GABA receptor activity that governs deep sleep stages. When cellular magnesium is insufficient, sleep architecture is disrupted regardless of hours in bed.
Fixing sleep without addressing the cellular inputs that enable restorative sleep is treating a downstream symptom.
Coenzyme Q10 acts as an electron carrier in the mitochondrial energy chain. CoQ10 production declines with age, with statin use, and with sustained oxidative stress. Its insufficiency compounds the cellular energy deficit described above.
DOES THIS APPLY TO YOU? If you have thyroid dysfunction, iron deficiency anaemia, sleep apnoea, or clinical depression, those conditions are the primary driver and require treatment. The cellular mechanism described above is the most common functional explanation for fatigue where clinical testing returns normal results. Both can coexist: clinical treatment addresses the condition, and cellular support addresses the energy deficit that often persists even after clinical treatment. |
Unlike vague promises of more energy, these are specific measurable outcomes to track across 30 days. If the cellular energy mechanism is the primary driver and you address it correctly, you should observe the following markers.
RESOLUTION CRITERIA: HOW YOU KNOW IT IS WORKING Track these four markers across 30 days:
|
These are not guaranteed outcomes for every individual. They are the markers that confirm the intervention is addressing the right mechanism. If fewer than two of these improve after 30 days of consistent protocol execution, escalate to further clinical investigation rather than continuing the same approach.
This is not a supplement list. It is a structured four-phase correction sequence. Each phase depends on the one before it.
PHASE 1 – ELIMINATE HIDDEN CLINICAL DRIVERS – WITHIN 7 DAYS
|
PHASE 2 – RESTORE CELLULAR INPUTS – 30 DAY MINIMUM
|
PHASE 3 – REDUCE ENERGY LEAKAGE – CONCURRENT WITH PHASE 2
|
PHASE 4 – EVALUATE RESPONSE – AT DAY 30
|
The morning sipping protocol delivers ionic minerals continuously through the hours of highest cortisol activity. For the full context of why mineral form and delivery matters, see our post on how mineral bioavailability affects what supplements actually do in the body.
If you are working on Phase 2 and want to address both the magnesium input and the cortisol buffer in parallel, these are the two mechanisms with the most direct relevance to the protocol above.
Standard Thinking | The Biological Reality |
|---|---|
You are tired because you are not sleeping enough | Waking tired despite adequate sleep is a cellular restoration problem. Sleep duration without the required cellular inputs does not produce restorative sleep |
A normal blood test means nothing is wrong | Standard tests measure serum mineral levels which the body maintains at all costs by drawing from tissue reserves. Normal serum does not confirm adequate cellular mineral status. Only 1 percent of body magnesium is in the blood |
Caffeine fixes low energy | Caffeine masks fatigue signals by blocking adenosine receptors. It does not produce ATP. The cellular depletion continues underneath the stimulation and compounds over time |
Fatigue means you need more rest | Fatigue from cellular depletion does not improve with rest alone. It improves when the depleted cellular inputs are restored. Rest without restoration inputs is not recovery |
Supplements are optional additions to an energy routine | Magnesium is required for ATP production. At cellular insufficiency this is not optional support. It is a missing input in a required biological process |
If your tests are normal and this pattern matches your experience, continuing to treat fatigue as a sleep or motivation issue will not resolve it. The problem is energy production at the cellular level. The four-phase protocol above addresses that directly.
Without correcting the cellular inputs, the pattern will persist regardless of how much sleep you get or how much caffeine you consume. The mechanism is biological. The correction is specific. The outcome is measurable within 30 days.
Persistent tiredness with normal blood tests is most commonly driven by cellular mineral depletion affecting mitochondrial ATP production, compounded by elevated cortisol from sustained stress and disrupted sleep architecture. Standard blood tests measure serum mineral levels which do not reflect cellular status. A GP blood panel is the right starting point to exclude clinical causes. If results are normal, the four-phase cellular correction protocol above is the most direct response.
Waking unrestored after adequate sleep hours is a signal that the restoration process during sleep is incomplete. The most common drivers are insufficient cellular magnesium disrupting GABA-mediated deep sleep stages, elevated cortisol fragmenting sleep architecture, and mitochondrial depletion that cannot be repaired overnight without the required inputs. Spending more hours in bed does not address any of these. Phase 2 and Phase 3 of the protocol above specifically target the restoration mechanisms.
Chronic fatigue as a persistent symptom requires clinical exclusion of conditions including chronic fatigue syndrome, thyroid dysfunction, anaemia, sleep apnoea, and depression. Where clinical causes are excluded, the most common functional explanation is cellular energy insufficiency driven by mineral depletion, sustained cortisol elevation, and compromised mitochondrial restoration during sleep. These are addressable through the protocol described above.
CoQ10 is required for the electron transport chain reactions that produce the majority of cellular ATP. Symptoms associated with CoQ10 insufficiency include fatigue, muscle weakness or aching, reduced exercise tolerance, and brain fog. CoQ10 production declines with age and with statin use. Dietary sources including oily fish and organ meats provide limited amounts. Supplementation is the more practical approach where insufficiency is suspected.
Magnesium is a required cofactor in ATP synthesis. Without adequate cellular magnesium, energy production is impaired at the biochemical level. The relevant distinction is between serum magnesium, which standard tests measure and which appears normal until severe depletion, and intracellular magnesium, which reflects actual cellular availability. Forms with higher bioavailability are generally preferred in research contexts for addressing cellular status.
ONE MORE THING BEFORE YOU GO If your fatigue pattern does not quite match what is described here, or if you have tried the protocol and want to talk through what the next step might be, leave it in the comments below. Tell us how long the fatigue has been present, what you have already tried, and which of the four resolution criteria you are seeing or not seeing. If your GP told you everything is normal but you are still exhausted, that is specifically the experience this post was written for. We read every comment and respond with what the research says about your specific situation. |
Legal Disclaimer
The information in this post is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. Persistent fatigue has many possible causes requiring individual assessment. Always seek personalised advice from a qualified healthcare provider before starting or changing any treatment or supplement regimen.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!



No products in the cart.