Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You are not dramatically ill. You do not have a diagnosed immune condition. But you are always a step behind. A cold that should last three days lasts ten. You pick up whatever is going around while others in the same room do not. You recover slowly, feel run down for longer than seems reasonable, and never quite reach the point of feeling fully well before the next thing arrives.
This is not bad luck. It is a pattern. And patterns have causes.
Our research indicates the most common driver of this chronic low-grade immune underperformance is not a lack of vitamin C or echinacea. It is a specific mineral deficit in the zinc and magnesium supply that immune cells require to produce, activate, and sustain an effective response. The mechanism is precise. The solution is specific. And neither looks like what most immune supplements are selling.
This is the question most people arrive with. Not a diagnosis. A suspicion. Something feels chronically off and they want to know whether what they are experiencing is actually an immune pattern or something else.
Here are the specific observable signs. Note how many apply to you consistently, not occasionally.
Frequency and recovery: You get sick more often than the people around you in similar environments. When you do get sick, recovery takes noticeably longer than it should. You feel run down for days or weeks after an illness that others shake in 48 hours. You have had the same infection or a similar one recur within a short period.
Persistent low-grade symptoms: You carry a baseline fatigue that does not lift even when you are not acutely ill. You feel like you are always fighting something, never fully well. Minor cuts or wounds take longer to heal than you would expect. You get cold sores, mouth ulcers, or skin flares that appear when you are stressed or run down.
Patterns that suggest suppressed immunity: Your immune responses feel delayed. You struggle with allergies or sensitivities that have worsened over time. You have been on antibiotics more than twice in the past twelve months.
If you recognise four or more of these patterns consistently rather than occasionally, the chronic immune underperformance pattern is likely. The question then is not whether your immune system is underperforming. It is why.
BEFORE YOU READ FURTHER This post describes one specific mechanism behind chronic immune underperformance: zinc and magnesium depletion reducing immune cell production and energy supply, compounded by cortisol suppression. This is a real and common mechanism. It is not the only one. See a healthcare provider before treating this as a mineral deficiency issue if: you have a diagnosed autoimmune condition, you are immunocompromised from medication or a medical condition, your immune challenges are severe rather than the low-grade chronic pattern described here, or you have experienced a sudden and significant decline in immunity rather than a gradual pattern. The mechanism described in this post is most relevant for otherwise healthy people experiencing a gradual, persistent pattern of immune underperformance. Mineral restoration supports immune function. It does not replace specialist management of diagnosed immune conditions. |
This is the question most people have before they have even articulated it. You eat vegetables. You try to eat well. Why would you be low in magnesium?
Two reasons. Neither is about your food choices.
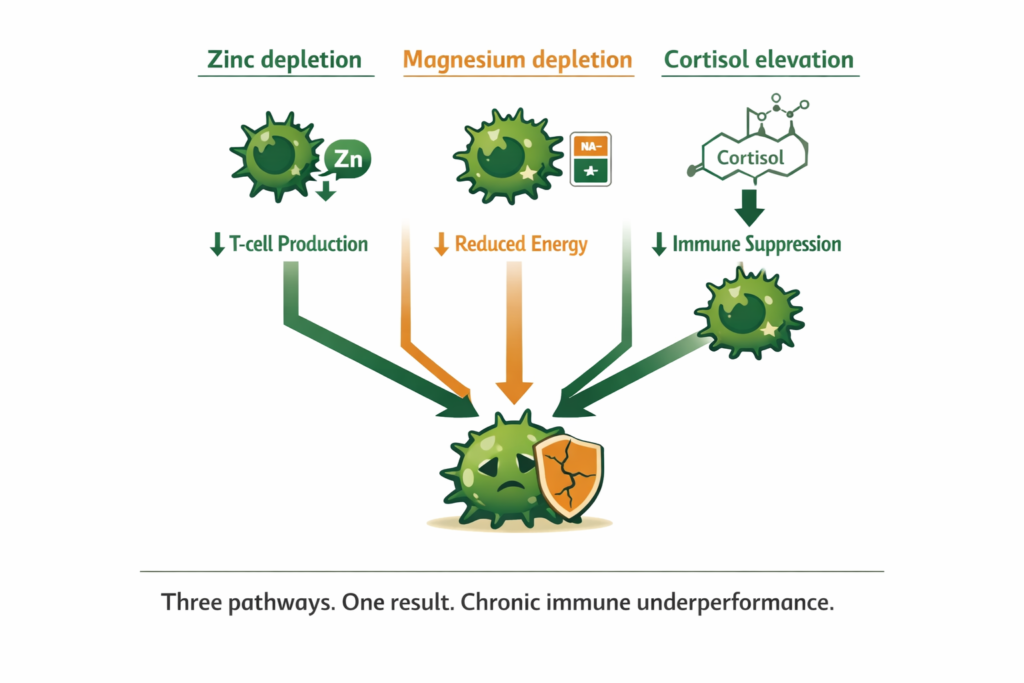
The zinc depletion pathway. Zinc is required for the production of T-cells in the thymus gland, the primary mechanism of the adaptive immune response. T-cells are what identify and eliminate pathogens. Without adequate zinc, the thymus cannot produce T-cells at the rate the body needs. The immune response is slow, weak, and often incomplete.
The magnesium depletion pathway. Every immune cell, like every other cell, runs on the sodium-potassium pump. The pump requires magnesium to operate. When magnesium is depleted, immune cells run at reduced capacity. Their ability to produce energy, replicate, and mount a sustained response is compromised. The immune system is not broken. It is underfuelled.
The cortisol suppression pathway. Chronic stress elevates cortisol. Elevated cortisol directly suppresses immune function as part of the emergency response, diverting resources toward immediate survival and away from long-term immune defence. If you notice you reliably get sick after periods of sustained stress, this is not coincidence. It is the cortisol-immunity mechanism expressing itself predictably.
DEFINITION T-CELLS T-cells are the primary cells of the adaptive immune response. They are produced in the thymus gland and are responsible for identifying pathogens and coordinating the body’s targeted immune response. Zinc is required for both T-cell production in the thymus and T-cell activation once produced. Without adequate zinc at the cellular level, both the speed and strength of the adaptive immune response are measurably reduced. |
WHAT TO DO ABOUT IT The three pathways share a common thread. All three are driven or accelerated by mineral depletion. Restoring ionic zinc and magnesium addresses the T-cell production mechanism and the immune cell fuel supply simultaneously. Reducing cortisol through adaptogenic support addresses the suppression signal. These are not separate interventions. They are the same intervention applied to the same root cause from different directions. |
WHAT TO DO ABOUT IT The three pathways share a common thread. All three are driven or accelerated by mineral depletion. Restoring ionic zinc and magnesium addresses the T-cell production mechanism and the immune cell fuel supply simultaneously. Reducing cortisol through adaptogenic support addresses the suppression signal. These are not separate interventions. They are the same intervention applied to the same root cause from different directions. |
Zinc is the mineral with the strongest and most specific clinical evidence for immune function. But the gap between what most people are taking and what their immune cells actually receive is the same gap we have seen in every other mineral context: the form determines the outcome.
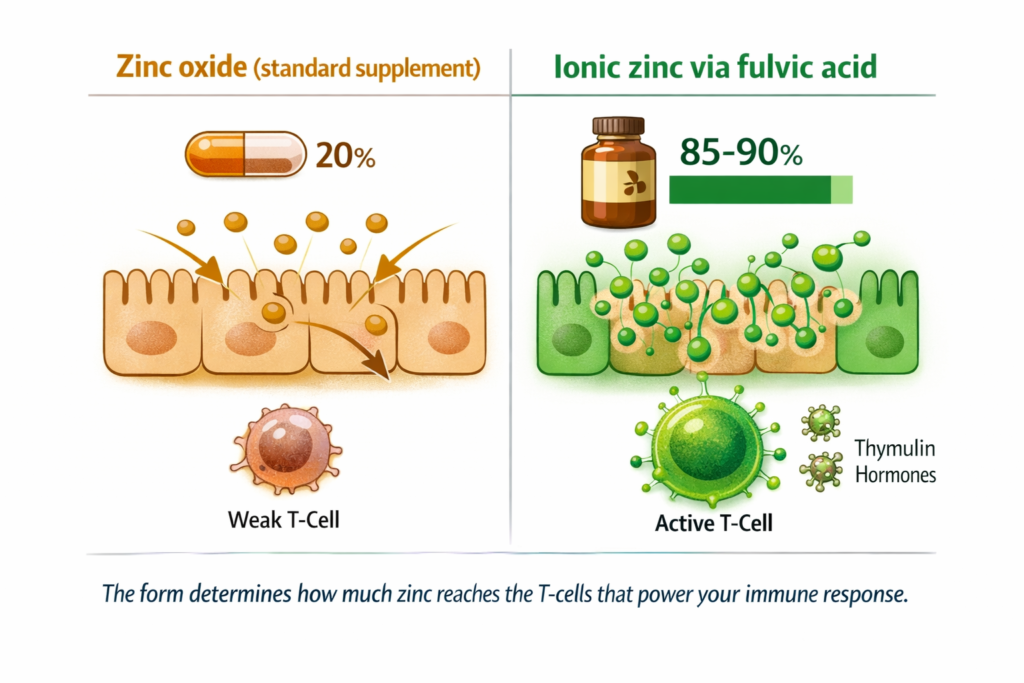
The zinc oxide in the majority of immune supplements and multivitamins absorbs at approximately 20 percent. From a 50mg tablet, your immune cells receive roughly 10mg of usable zinc. Zinc picolinate absorbs at 40 to 60 percent. Ionic zinc via fulvic acid achieves 80 to 90 percent. From the same stated 50mg, your immune cells receive 40 to 45mg. T-cell production in the thymus is directly proportional to zinc availability at the cellular level. The gap between 10mg and 45mg reaching the cell is the gap between a marginal immune response and a functional one.
DEFINITION THYMUS GLAND The thymus is the organ in the chest where T-cells mature and are prepared for immune defence. It requires zinc to produce the hormone thymulin, which drives T-cell maturation. Without adequate intracellular zinc, thymulin production drops, T-cell maturation is impaired, and the adaptive immune response loses both speed and specificity. This is why zinc deficiency at the cellular level produces immune impairment even when blood zinc levels appear within normal range. |
WHAT TO DO ABOUT IT The ionic form of zinc matters here specifically because T-cells in the thymus require zinc in its electrically charged, dissolved state to use it directly. The same fulvic acid transport mechanism that carries ionic magnesium across cell membranes carries ionic zinc to the same cells. If you have taken zinc supplements before and noticed limited immune benefit, the form and the absorption ceiling are the variables to address before the dose. |
DOES THIS APPLY TO YOU? If you have taken zinc supplements during illness and noticed they helped some but not dramatically, you were almost certainly absorbing a fraction of the stated dose. If you regularly take a multivitamin that lists zinc oxide and wonder why your immunity has not improved, the 20 percent absorption ceiling is the explanation. The dose on the label is not the dose your T-cells receive. |
Immune function is metabolically expensive. Producing T-cells, activating white blood cells, sustaining an inflammatory response, and mounting the cellular machinery of defence all require significant energy production. That energy is produced by the same sodium-potassium pump mechanism that powers every other cellular process. When magnesium is depleted, immune cells are underfuelled. They can still respond, but the response is slower, weaker, and shorter-lived.
There is a second magnesium-immunity connection that is less discussed. Magnesium is required for the production of glutathione, the body’s primary antioxidant. Glutathione protects immune cells from the oxidative stress of their own activity during an infection response. Without adequate magnesium to support glutathione production, immune cells burn out faster during a response, shortening both the duration and the effectiveness of the fight. This is the mechanism behind the slow, incomplete recovery pattern many people experience after illness.
WHAT TO DO ABOUT IT The morning sipping protocol delivers ionic magnesium continuously through the hours of highest demand, keeping immune cell fuel supply consistent throughout the day. Adequate magnesium also supports sleep quality, and sleep is when the immune system conducts its primary maintenance and regeneration processes. Magnesium deficiency disrupting sleep disrupts immune maintenance simultaneously. |
DOES THIS APPLY TO YOU? If your recovery from illness is consistently slow, meaning the acute phase passes but you feel run down for a disproportionate period afterward, the glutathione depletion mechanism is likely part of what you are experiencing. Immune cell recovery after a response requires magnesium. If that supply is insufficient, the post-illness fatigue persists longer than it should. If you also experience poor sleep alongside your immune challenges, the connection is almost certainly active. |
We cover the full magnesium depletion mechanism and the symptom pattern it produces in our post on symptoms of magnesium deficiency and what your body is actually missing.
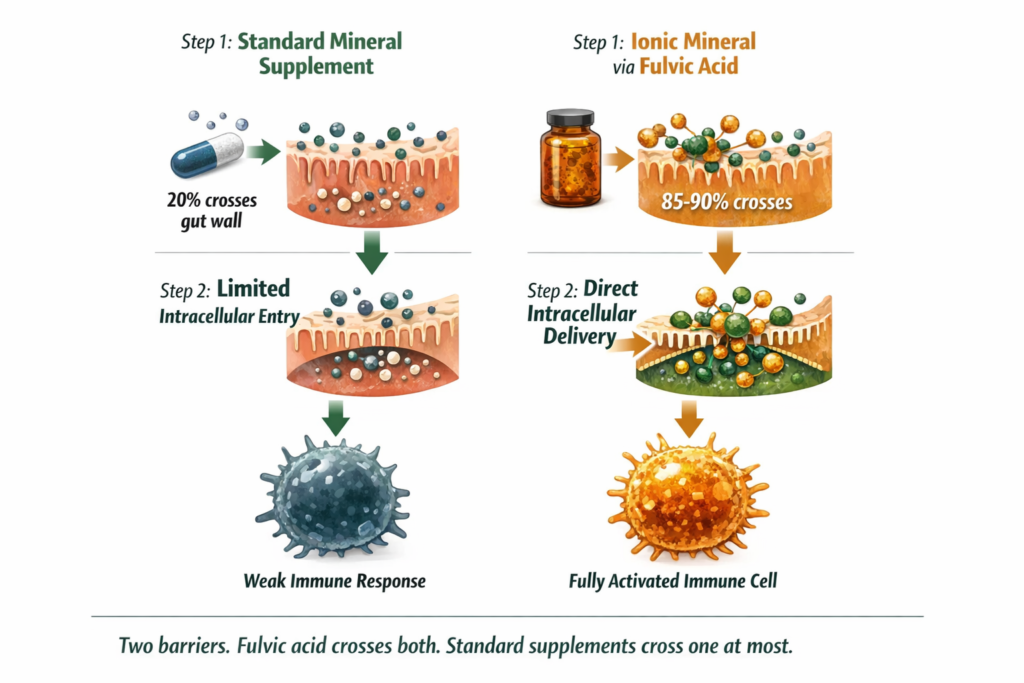
Most immune supplements deliver their active minerals through standard gut absorption pathways. The mineral dissolves in the gut, crosses the gut wall through passive diffusion or carrier-mediated transport, enters the bloodstream, and then needs to cross the cell membrane to reach the intracellular environment where immune function actually happens. Every step in this pathway has an efficiency ceiling.
Fulvic acid changes the equation at both steps. At the gut wall: fulvic acid actively transports ionic minerals across rather than relying on passive diffusion. This is what produces the 80 to 90 percent absorption figure for ionic zinc versus 20 percent for zinc oxide. At the cell membrane: fulvic acid carries ionic minerals directly through cell membranes into the intracellular environment where T-cell production and immune function occur. Zinc and magnesium that reach the inside of immune cells produce an immune response. Zinc and magnesium that circulate in the blood but do not efficiently cross cell membranes produce a better-looking blood test, not a better immune response.
WHAT TO DO ABOUT IT Ashwagandha modulates the HPA axis feedback sensitivity, reducing the degree to which sustained stress translates into sustained cortisol elevation. When cortisol returns toward its natural rhythm, immune suppression from the cortisol pathway lifts. This is why ashwagandha appears in both the stress literature and the immune health literature. It is the same mechanism addressing immune suppression from the hormonal side while ionic mineral restoration addresses it from the mineral supply side. |
DOES THIS APPLY TO YOU? If your immune challenges cluster around periods of high workload, relationship stress, or major life change rather than being random and constant, the cortisol suppression pathway is the dominant mechanism. Zinc and magnesium restoration addresses the mineral depletion cortisol causes. Ashwagandha addresses the suppression signal itself. If stress is your primary driver, also consider whether the stress itself warrants direct support. Mineral and adaptogenic supplementation addresses the biological consequence of chronic stress. It does not address the source. Both the biological impact and the source are worth attending to simultaneously. |
Cortisol suppresses immune function as a feature, not a bug. In the emergency response, the body prioritises immediate survival and deprioritises long-term maintenance. Immune defence is a long-term maintenance process. It is expensive, it is not immediately necessary in a crisis, and it is the first thing the cortisol signal turns down.
Cortisol specifically reduces T-cell production and activity, reduces natural killer cell activity, reduces antibody production, and increases the threshold at which the immune system mounts a response. These are not vague effects of general stress. They are measurable consequences of the cortisol signal. Chronic stress means chronic cortisol elevation. Chronic cortisol elevation means chronic immune suppression. It runs alongside the mineral depletion pattern because cortisol also depletes zinc and magnesium with each activation, compounding the immune impact from two directions simultaneously.
The full cortisol mechanism and how to break the depletion cycle are covered in our post on high cortisol symptoms and what actually breaks the cycle.
WHAT TO DO ABOUT IT Ashwagandha modulates the HPA axis feedback sensitivity, reducing the degree to which sustained stress translates into sustained cortisol elevation. When cortisol returns toward its natural rhythm, immune suppression from the cortisol pathway lifts. This is why ashwagandha appears in both the stress literature and the immune health literature. It is the same mechanism addressing immune suppression from the hormonal side while ionic mineral restoration addresses it from the mineral supply side. |
DOES THIS APPLY TO YOU? If your immune challenges cluster around periods of high workload, relationship stress, or major life change rather than being random and constant, the cortisol suppression pathway is the dominant mechanism. Zinc and magnesium restoration addresses the mineral depletion cortisol causes. Ashwagandha addresses the suppression signal itself. If stress is your primary driver, also consider whether the stress itself warrants direct support. Mineral and adaptogenic supplementation addresses the biological consequence of chronic stress. It does not address the source. Both the biological impact and the source are worth attending to simultaneously. |
Standard Thinking | The Biological Reality |
|---|---|
Take vitamin C when you feel a cold coming | Vitamin C supports immune function but does not address the zinc deficit in T-cell production or the magnesium deficit in immune cell energy supply that drives the chronic underperformance pattern |
Zinc is zinc, any form will do | Zinc oxide absorbs at 20 percent. Ionic zinc via fulvic acid absorbs at 80 to 90 percent. The form determines how much reaches the T-cells where it is needed |
Stress makes you more likely to get sick | Cortisol specifically reduces T-cell production and activity through a measurable biological mechanism. Stress suppresses immunity precisely and predictably, not vaguely |
If you eat well your immune system should be fine | Modern soil depletion means food zinc and magnesium content is a fraction of what it was in previous generations. Eating well is necessary but no longer sufficient as a sole mineral strategy |
Getting sick frequently is just bad luck | Frequent illness and slow recovery are predictable downstream effects of a specific mineral and hormonal pattern: zinc depletion reducing T-cell production, magnesium depletion reducing immune cell energy, and cortisol suppression reducing immune activation |
The most consistent signs are getting sick more frequently than those around you in similar environments, recovering more slowly than expected, feeling run down for a prolonged period after illness, recurring infections such as cold sores or throat infections, slow wound healing, and a persistent baseline fatigue that does not lift between illness episodes. These signs reflect chronic immune underperformance driven by zinc and magnesium depletion reducing T-cell production and immune cell energy supply, often compounded by cortisol elevation suppressing immune activation through the stress pathway.
Zinc is required for T-cell production in the thymus and T-cell activation once produced. T-cells are the primary cells of the adaptive immune response that identify and eliminate pathogens. Zinc is also required for the production of thymulin, the hormone that drives T-cell maturation. Without adequate intracellular zinc, both the speed and strength of the adaptive immune response are measurably reduced. The form of zinc supplementation determines how much reaches the intracellular environment where T-cell production occurs: ionic zinc via fulvic acid achieves 80 to 90 percent intracellular delivery versus 20 percent for the zinc oxide in most standard supplements.
Yes, through a direct and measurable biological mechanism. Cortisol reduces T-cell production and activity, reduces natural killer cell activity, reduces antibody production, and raises the threshold at which the immune system mounts a response. These are specific consequences of the cortisol signal, not indirect effects of general wellbeing. Chronic stress means chronic cortisol elevation which means chronic immune suppression. Cortisol also depletes zinc and magnesium with each activation, compounding the immune impact from two directions simultaneously. Adaptogenic support that modulates HPA axis feedback reduces the degree to which sustained stress translates into sustained immune suppression.
The most common explanations are form and intracellular delivery. Zinc oxide in most supplements absorbs at 20 percent, meaning a 50mg tablet delivers approximately 10mg of usable zinc. That is insufficient to meaningfully support T-cell production. Even better-absorbed forms like zinc picolinate may reach the bloodstream efficiently but face a second barrier at the cell membrane. Ionic zinc carried by fulvic acid crosses both barriers, reaching the intracellular environment where immune function actually occurs. If you have tried zinc and magnesium supplements without meaningful immune improvement, the intracellular delivery step is almost certainly the variable that has not been addressed.
Meaningful improvement in immune function typically emerges over four to six weeks of consistent ionic zinc and magnesium supplementation. T-cell production in the thymus responds to zinc availability over weeks rather than days. The fastest-responding effects are typically reduced severity of acute illness rather than reduced frequency, which follows as zinc and magnesium reserves are restored to adequate cellular levels. Frequency reduction typically becomes noticeable over two to three months of consistent use alongside the reduced cortisol burden that adaptogenic support provides.
ONE MORE THING BEFORE YOU GO If something in this post resonated but left a question unanswered, leave it in the comments below. We read every comment and respond with what the research says. If your immune pattern does not fully match what is described here, tell us specifically what is different. You will get a direct research-based response. We are not asking you to engage for the sake of it. We are giving you a direct line to a researched answer on anything this post did not fully close for your situation. |
Legal Disclaimer The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are experiencing persistent or severe symptoms including frequent heart palpitations, severe muscle weakness, or significant mood disturbance, consult a qualified healthcare provider.
Never Miss any Updates From Blog!




No products in the cart.