Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
Do not stop filtering. Contaminant removal matters. Add the ionic minerals back after filtration. Here is the specific method:
Take your filtered water storage container, whether that is a 5 litre jug, a 10 litre tank, or a countertop dispenser. Add ionic mineral concentrate drops to the filtered water before drinking. A standard ionic mineral concentrate delivers approximately 75 to 125 mg of combined ionic minerals per recommended dose. For a 5 litre container, a standard dose of 20 drops of a quality ionic mineral concentrate will raise TDS by approximately 50 to 80 PPM depending on the product concentration. Test with your TDS meter after adding minerals and adjust the dose until the reading reaches 150 to 250 PPM. This is your calibrated dose. Apply it consistently every time you refill.
Important: use a genuine ionic mineral concentrate, not a colloidal mineral product. Ionic minerals are fully dissolved and electrically charged. Colloidal minerals are suspended particles. The gut transports the ionic form efficiently. The colloidal form requires the same conversion process as other particulate supplements and achieves significantly lower absorption.
You drink water every day. You probably drink more than most people. You may have even invested in a quality filtration system to remove the contaminants your tap water carries. You are doing what every health recommendation tells you to do. And yet something is still not working the way it should. Energy that does not hold across the day. Muscles that cramp without explanation. Sleep that does not fully restore. A cognitive sharpness that comes and goes with no identifiable cause.
The blood test comes back normal. Your doctor says you are fine. The minerals are there. The numbers say so.
But your cells disagree. And the reason they disagree has nothing to do with how much water you drink. It has everything to do with what that water no longer contains, and what your food stopped delivering decades before you were born.
Our research indicates the most consistent and overlooked variable in chronic subclinical fatigue, muscle dysfunction, and poor sleep quality is not a missing supplement or an undiagnosed condition. It is an ionic mineral gap: the measurable distance between the mineral environment your biology was designed to operate in and the mineral environment modern food and water actually provides.
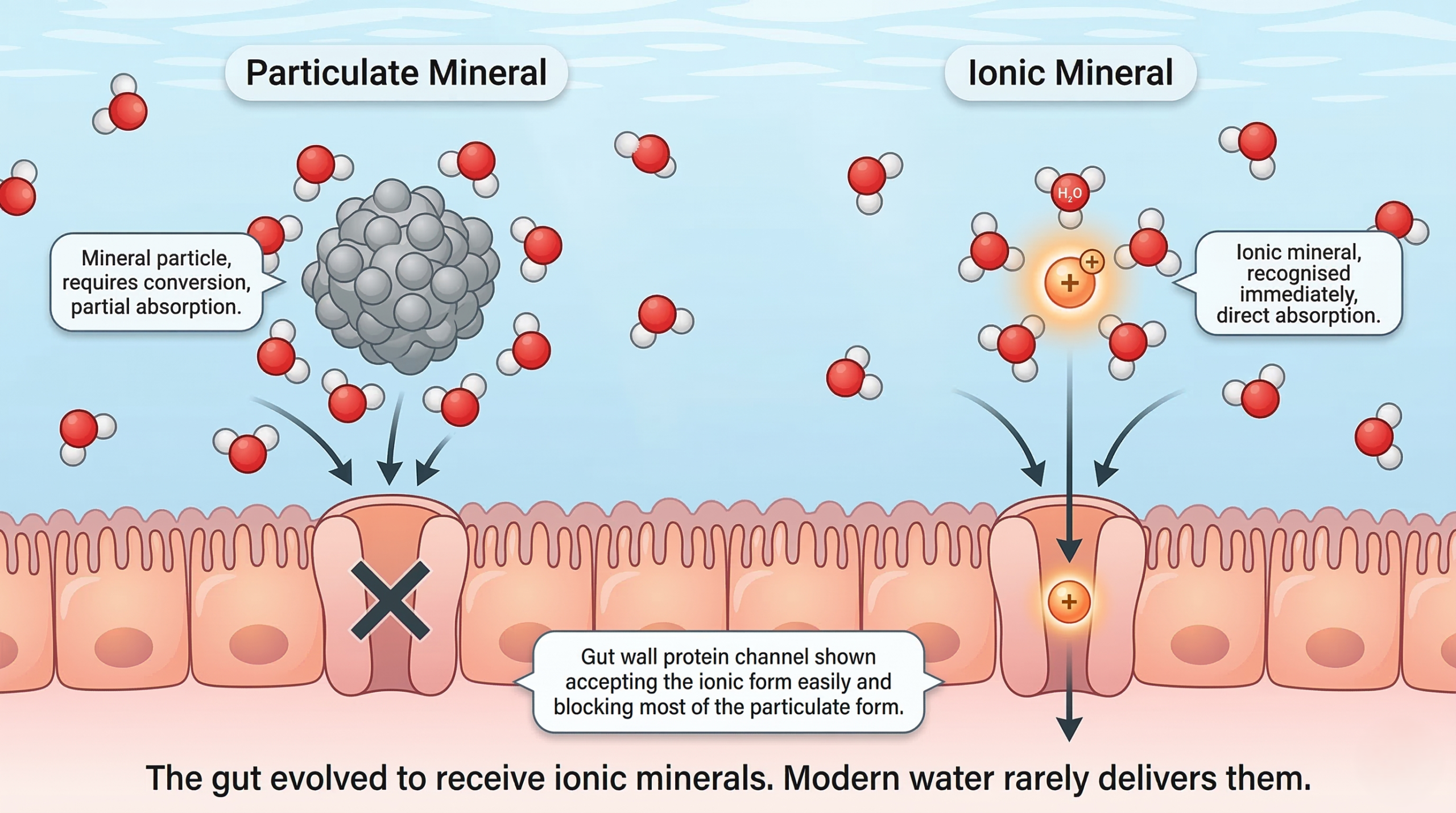
Not all minerals in food and water behave identically in the body. A mineral particle suspended in water is physically different from a mineral that has dissolved completely into its ionic, electrically charged state. The distinction is not a technicality. It determines whether the mineral can be recognised and transported by the biological systems designed to use it.
Ionic minerals are single atoms that have lost or gained electrons, giving them a positive or negative electrical charge. In this state they are fully dissolved, invisible to the naked eye, and recognised directly by the protein channels in the gut wall and cell membranes that evolved specifically to transport them. No digestion required. No conversion required. The gut sees the charge and moves the mineral through.
Think of it like a key cut to fit a specific lock. The ionic form is the correctly cut key. Mineral particles, mineral complexes from poorly formulated supplements, and minerals bound in insoluble compounds are keys with the wrong cut. Some will eventually work with enough force. Many will not work at all. The gut processes what it can and passes the rest through.
Natural spring water that has traveled through mineral-rich geological rock formations over centuries delivers minerals already in the ionic state. The rock dissolves slowly into the water. The minerals arrive in solution, charged, ready for immediate biological use. This is the form human biology co-evolved with over millions of years of drinking from natural water sources. It is also the form that modern water systems, whether reverse osmosis filtration, municipal chlorination, or standard bottled water, largely fail to deliver.
Total Dissolved Solids, measured in parts per million and abbreviated as TDS, is the standard measurement for how much dissolved mineral content water carries. It is the most accessible proxy for ionic mineral delivery available to a consumer without laboratory equipment. A TDS meter costs under fifteen dollars and gives a reading in seconds.
Did You Know: What is TDS?
Total Dissolved Solids is a measure of all dissolved substances in water, primarily minerals like calcium, magnesium, potassium, and sodium. A TDS reading tells you how mineralised your water is. It does not tell you which minerals are present or in what ratio, but it gives you an immediate indication of whether your water is carrying meaningful ionic mineral content or delivering essentially nothing. [Read our full TDS explanation in The Purity Paradox: Read blog]
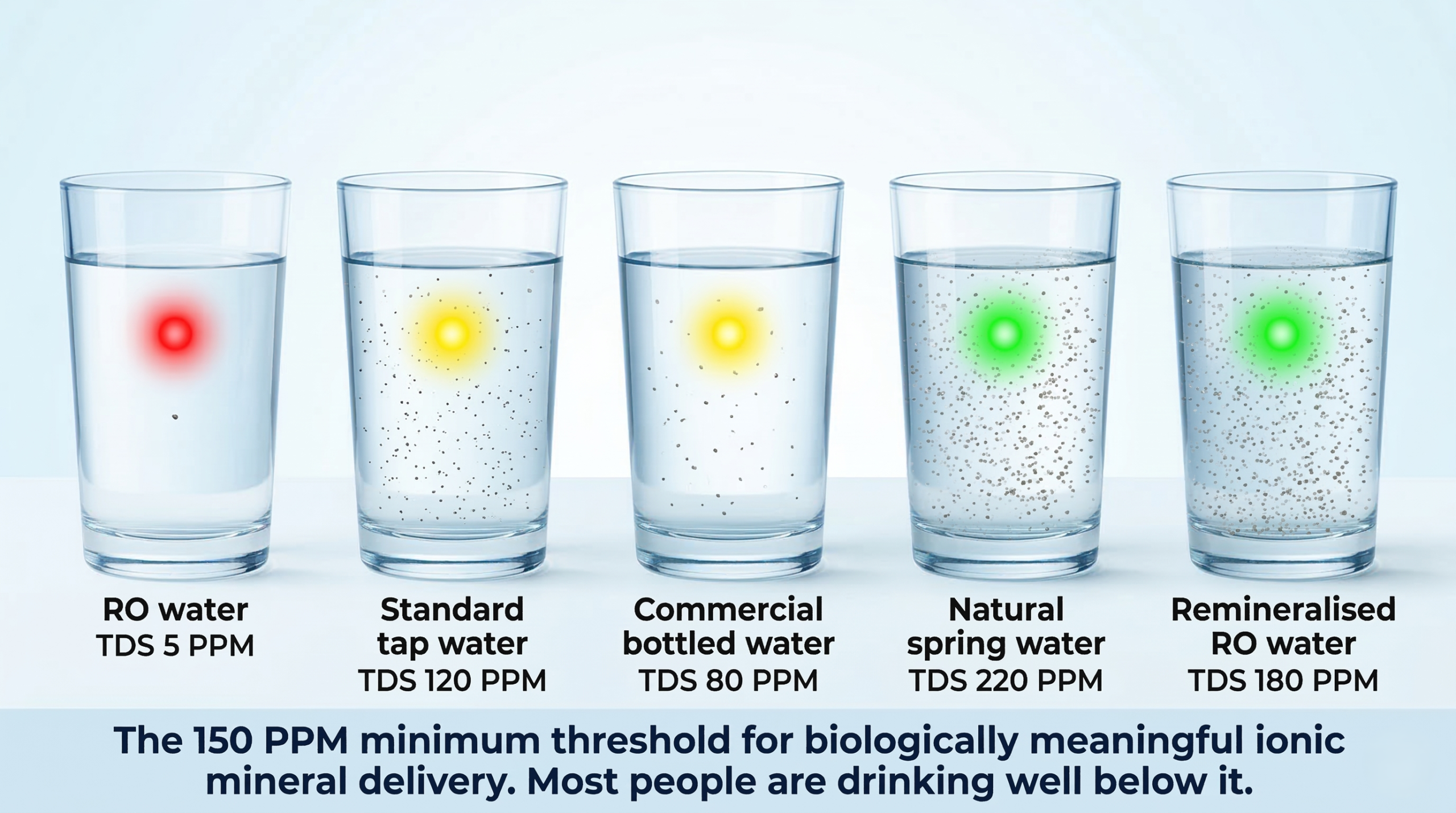
The research-supported minimum TDS for water to carry biologically meaningful ionic mineral content is 150 PPM. Natural spring water from mineral-rich geological sources typically reads between 150 and 300 PPM. Some therapeutic mineral waters, used clinically in European spa medicine for centuries, read between 300 and 1,000 PPM depending on the geological source.
Water Source | Typical TDS Range (PPM) | Ionic Mineral Delivery | Biological Adequacy |
|—|—|—|—|
| Reverse osmosis filtered water | 0 to 10 | Near zero | Inadequate |
| Standard tap water (varies by region) | 50 to 500 | Variable, often low ionic fraction | Inconsistent |
| Most commercial bottled water | 30 to 150 | Low to marginal | Often inadequate |
| Natural spring water (geological source) | 150 to 300 | Good ionic mineral content | Adequate |
| Therapeutic mineral water (European spa standard) | 300 to 1,000 | High ionic mineral content | Optimal for therapeutic use |
| Remineralised RO water with ionic concentrate | 150 to 250 | Restored ionic mineral content | Adequate when correctly dosed |
A person drinking reverse osmosis filtered water is consuming water with a TDS of 0 to 10 PPM. The target is 150 PPM minimum. That gap is not a minor nutritional shortfall. It represents the near-complete removal of a mineral delivery mechanism the body has relied on throughout its evolutionary history, replaced with nothing.
**Did You Know: What is Reverse Osmosis?
> Reverse osmosis is a water filtration method that forces water through a semi-permeable membrane, removing contaminants, heavy metals, bacteria, and dissolved solids. It produces very clean water but also removes beneficial minerals in the process, leaving TDS readings of 0 to 10 PPM. [Read our full breakdown in Beyond the Filter: link]
The water gap is one half of the problem. The food gap is the other, and it has been building since the 1950s.
Did You Know: What is Soil Mineral Depletion?**
> Industrial farming practices introduced after World War Two replaced organic composting with synthetic fertilisers. Synthetic fertilisers feed crops nitrogen, phosphorus, and potassium but do not replenish the full spectrum of trace minerals the soil previously contained. Over decades, mineral density in food has declined measurably. [This was explained in detail in our Mineral Bioavailability post: link]
Research published in the Journal of the American College of Nutrition analysed USDA nutritional data for 43 garden crops between 1950 and 1999 and found consistent, significant declines across multiple minerals (Davis et al., 2004). These are not marginal differences. They represent a structural reduction in the ionic mineral load arriving from food, even for people eating what would be considered a high-quality diet.
| Vegetable | Calcium Decline | Iron Decline | Magnesium Decline | Zinc Decline |
|—|—|—|—|—|
| Broccoli | 63% | 34% | 24% | Not measured |
| Spinach | 10% | 27% | 10% | Not measured |
| Carrots | 48% | 80% | 75% | Not measured |
| Tomatoes | 62% | 73% | Not measured | Not measured |
| Potatoes | 35% | 55% | Not measured | 18% |
| Wheat (flour) | 28% | 19% | 15% | 10% |
Source: Davis, Epp and Riordan, 2004. Journal of the American College of Nutrition.
A person eating broccoli today receives 63 percent less calcium from the same serving size than their grandparents received in 1950. Not because the broccoli looks different. Because the soil it was grown in no longer contains the mineral density it once did.
Combined with the water gap, this creates a compound ionic mineral deficit that operates silently across every system in the body simultaneously, not dramatic enough to appear on standard diagnostic panels, consistent enough to undermine daily biological performance.
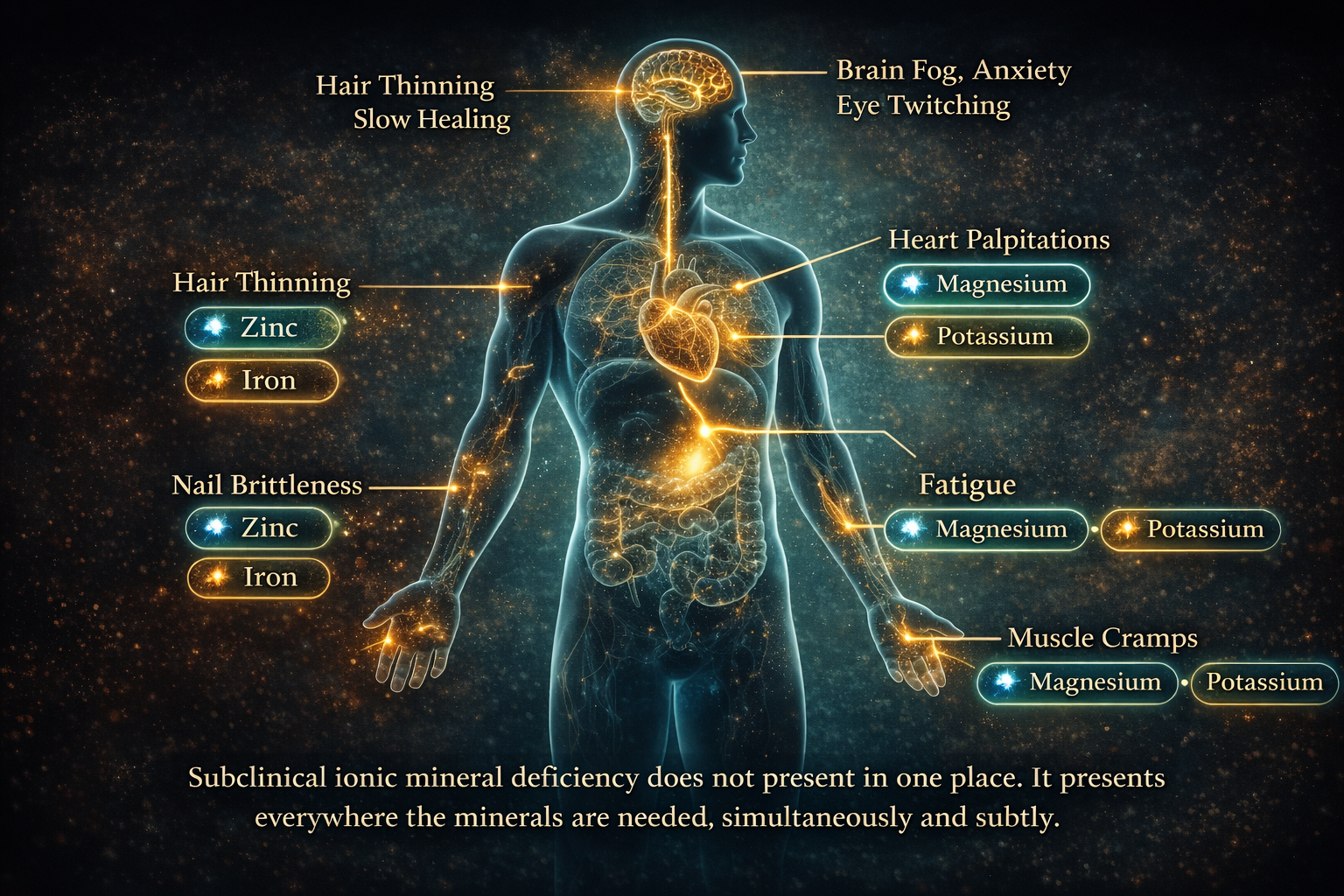
The symptoms of ionic mineral deficiency are not the dramatic presentation of acute deficiency disease. Acute magnesium deficiency produces seizures. Acute zinc deficiency produces severe immune failure. Those are clinical emergencies. They are not what most people experience.
**Subclinical ionic mineral deficiency** presents as the chronic low-grade symptoms that most people have normalised as part of modern life. They are consistent enough to be present most days, subtle enough that no single symptom points to a clear cause, and collectively significant enough to measurably reduce quality of life and biological performance.
> **Did You Know: What is the Sodium-Potassium Pump?**
> The sodium-potassium pump is a protein in every cell membrane that uses ionic minerals, specifically sodium and potassium, to maintain an electrical charge across the cell membrane. This charge powers aquaporin channels that allow water into the cell and drives the energy production cycle in mitochondria. When ionic mineral delivery is insufficient, the pump operates below capacity and every cell function that depends on it degrades accordingly. [Full explanation in our Cellular Hydration Pillar post: link]
| Symptom | Most Likely Mineral Gap | Why the Connection Exists |
|—|—|—|
| Muscle cramps, especially at night | Magnesium, Potassium | Both required for muscle relaxation after contraction. Deficiency leaves muscles unable to fully release |
| Fatigue that sleep does not resolve | Magnesium, Iron, Zinc | Magnesium required for ATP synthesis. Iron required for oxygen transport. Zinc required for mitochondrial enzyme function |
| Brain fog and cognitive inconsistency | Magnesium, Zinc | Both required for synaptic transmission and neurological signalling. Deficiency produces inconsistent cognitive performance |
| Poor sleep architecture, early waking | Magnesium | Required for GABA receptor function. Low magnesium produces light, non-restorative sleep without affecting ability to fall asleep initially |
| Eye twitching | Magnesium | Involuntary muscle fasciculation is a classic early magnesium deficiency presentation |
| Heart palpitations | Magnesium, Potassium | Both regulate cardiac electrical activity. Deficiency produces awareness of heartbeat and irregular rhythm perception |
| Slow wound healing | Zinc | Required for collagen synthesis and immune cell function. Deficiency slows tissue repair measurably |
| Hair thinning and nail brittleness | Zinc, Iron, Silica | All three required for keratin production and hair follicle integrity |
| Anxiety and nervous tension | Magnesium | Acts as a natural NMDA receptor antagonist. Low magnesium increases neurological excitability |
| Loss of taste or smell | Zinc | Zinc is the primary cofactor for the enzymes governing taste and olfactory function |
| Skin rashes and slow healing skin | Zinc | Zinc deficiency has a documented dermatological presentation including perioral rash and wound healing failure |
This table is a diagnostic starting point, not a clinical tool. Each symptom has multiple potential causes. But if three or more of these symptoms are present simultaneously without a clear diagnosed cause, ionic mineral delivery is a rational and well-evidenced variable to investigate.
This is the section most people need to read before they conclude that their minerals are fine.
Standard blood panels measure **serum mineral levels**: the concentration of minerals dissolved in the liquid portion of the blood. Serum magnesium, serum zinc, serum calcium. These measurements are accurate. They do reflect the mineral concentration in the bloodstream at the time of the test.
What they do not measure is **intracellular mineral status**: the concentration of minerals inside the cells where they are biologically active.
The body maintains serum mineral levels within a narrow range through a regulatory system that draws on bone, muscle, and tissue mineral reserves when dietary intake is insufficient. The purpose of this system is to protect the brain and heart from the consequences of acute mineral shortage. It does this effectively. Your serum magnesium will read normal until your tissue reserves are significantly depleted.
A person with chronically low dietary ionic mineral intake and compromised cellular delivery may show normal serum mineral levels while their cells are operating on progressively depleted reserves. The blood test reports normal. The cells report otherwise. This is not a flaw in the testing system. It is a measurement of the wrong compartment for the question being asked.
Did You Know: The Serum vs. Cellular Distinction**
> Only 1 percent of total body magnesium is found in the blood. The remaining 99 percent is stored in bone, muscle, and soft tissue. A serum magnesium test measures the 1 percent fraction the body maintains at all costs. It is a measure of the body’s mineral emergency management system, not of the mineral status in the cells where fatigue, sleep quality, and muscle function are actually determined (Workinger et al., 2018).
The test that more accurately reflects cellular mineral status is the red blood cell mineral test, also known as the intracellular mineral panel, which measures mineral concentration inside red blood cells rather than in the serum surrounding them. This test is not standard in routine blood work. Most people never receive it. Most practitioners do not order it unless specifically prompted.
Feature | Serum Mineral Test | Red Blood Cell (Intracellular) Test |
|—|—|—|
| What it measures | Mineral in blood plasma | Mineral inside red blood cells |
| Reflects dietary intake | Only after severe depletion | Within weeks of intake change |
| Reflects cellular status | No | Yes |
| Ordered routinely | Yes | Rarely |
| Cost | Standard | Higher, often not covered |
| When it reads low | Emergency depletion only | Early to moderate deficiency |
| Clinical use | Acute deficiency detection | Functional mineral status assessment
| Standard Industry Thinking | The Penantia Interpretation |
|—|—|
| If your blood test is normal, your minerals are fine | Serum tests measure the wrong compartment. Intracellular mineral status can be depleted while serum reads normal |
| Clean filtered water is the healthiest water | RO water at 0 to 10 PPM TDS delivers no ionic minerals. Clean is necessary. Mineralised is also necessary. They are not the same thing |
| Modern food provides all the minerals you need | Calcium in broccoli is down 63 percent since 1950. The food looks identical. The mineral delivery does not |
| Mineral supplements close the gap | Only if the form is ionic or chelated and the fulvic acid transport mechanism is present to deliver them to cells. Form and transport both matter |
| Fatigue and brain fog are lifestyle problems | They are frequently subclinical ionic mineral deficiency presenting in the exact tissues that depend most on continuous ionic mineral delivery |
| Drink more water | Drink mineralised water. Volume without ionic mineral content does not address the gap |
“Humans have been living on modern food and filtered water for decades without widespread mineral deficiency disease. If this gap were real, we would see it clearly in population health data.”
We do see it. It presents as the chronic disease burden that defines modern Western healthcare: cardiovascular disease, type 2 diabetes, osteoporosis, anxiety disorders, and sleep dysfunction are all conditions with documented associations with subclinical mineral deficiency, particularly magnesium, zinc, and calcium (DiNicolantonio et al., 2018). These are not presented clinically as mineral deficiency diseases because the regulatory and diagnostic framework does not use that framing. They are diagnosed and treated as independent conditions. The mineral foundation they share goes unaddressed.
The second part of the answer is that dramatic acute deficiency diseases, scurvy, rickets, pellagra, these appeared when a single nutrient was completely absent from the diet. The modern ionic mineral gap is not complete absence. It is persistent subclinical insufficiency across multiple minerals simultaneously. The body compensates through its reserve system. The consequences appear as chronic reduced function rather than acute disease. They are real, measurable, and consistently underattributed.
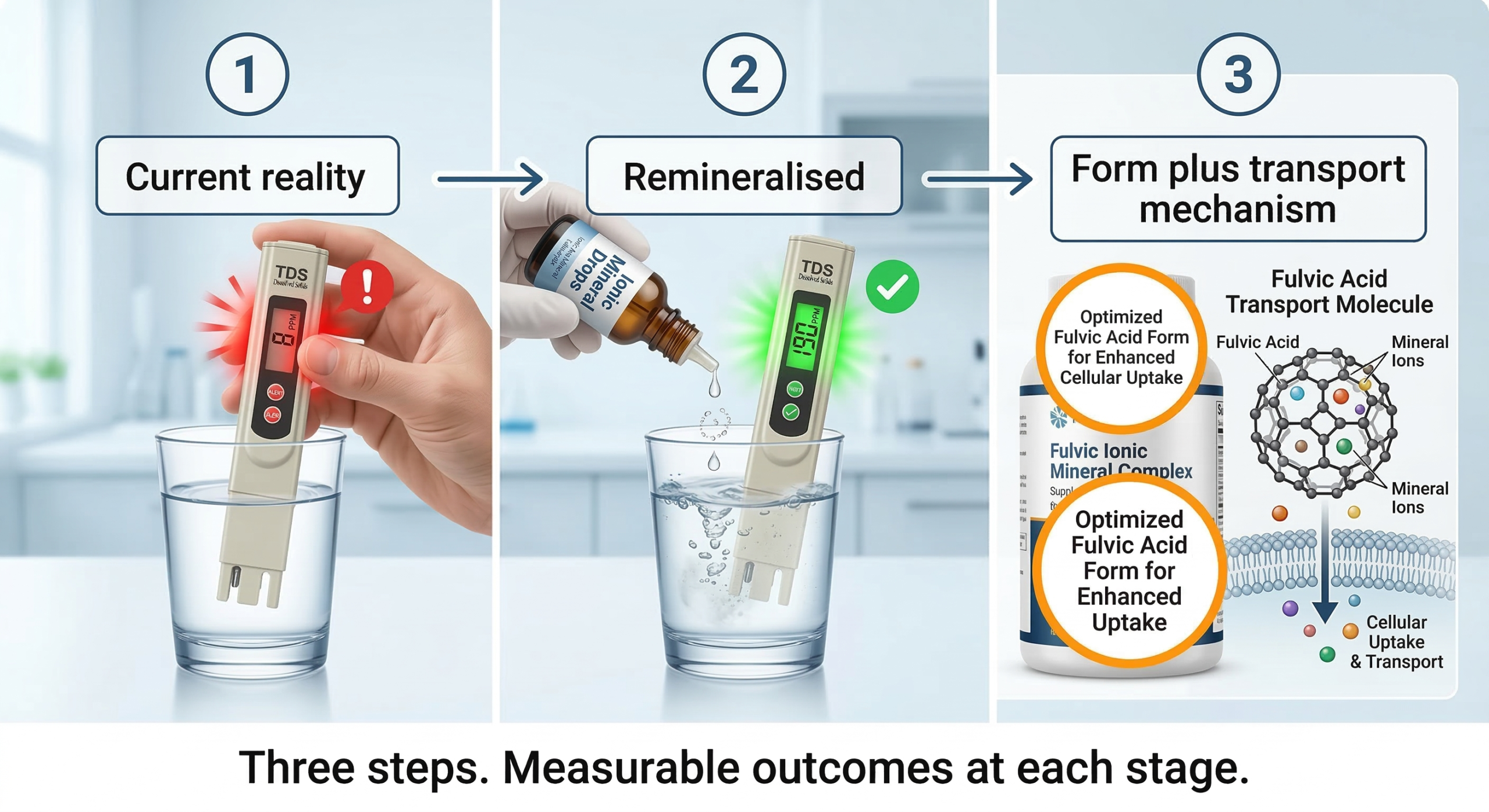
Understanding the ionic mineral gap is useful only if it leads to action. Here is the specific three-step protocol based on our research.
Did You Know: What is Fulvic Acid and why does it matter here?**
> Fulvic acid is the biological transport mechanism that carries ionic minerals across the gut wall and cell membrane. Restoring ionic mineral intake without also restoring the transport mechanism produces incomplete results. [Full explanation in The Fulvic Acid Blueprint: link]
Purchase a TDS meter. They are available online for under fifteen dollars. Fill a glass from your normal drinking water source and test it. If the reading is below 150 PPM you have confirmed an ionic mineral gap in your water supply. Write the number down.
Do not stop filtering. Contaminant removal matters. Add the ionic minerals back after filtration. Here is the specific method:
Take your filtered water storage container, whether that is a 5 litre jug, a 10 litre tank, or a countertop dispenser. Add ionic mineral concentrate drops to the filtered water before drinking. A standard ionic mineral concentrate delivers approximately 75 to 125 mg of combined ionic minerals per recommended dose. For a 5 litre container, a standard dose of 20 drops of a quality ionic mineral concentrate will raise TDS by approximately 50 to 80 PPM depending on the product concentration. Test with your TDS meter after adding minerals and adjust the dose until the reading reaches 150 to 250 PPM. This is your calibrated dose. Apply it consistently every time you refill.
Important: use a genuine ionic mineral concentrate, not a colloidal mineral product. Ionic minerals are fully dissolved and electrically charged. Colloidal minerals are suspended particles. The gut transports the ionic form efficiently. The colloidal form requires the same conversion process as other particulate supplements and achieves significantly lower absorption.
If you are supplementing minerals, apply the form hierarchy from Post 4. Glycinate and ionic forms over oxide and carbonate. Take with the appropriate cofactors, vitamin C with iron, vitamin D with calcium. Time magnesium and zinc separately to avoid gut transporter competition.
Then address the transport mechanism. Post 5 covers fulvic acid in detail. The short version: ionic minerals that reach the bloodstream still require fulvic acid to cross cell membranes and enter the cellular environment where they are biologically active. Restoring ionic mineral intake without restoring the transport mechanism addresses one barrier but not both.
Did You Know: What is the Mineral Form Hierarchy?**
> Oxide and carbonate forms of minerals deliver 4 to 22 percent absorption. Chelated forms like glycinate and malate deliver 40 to 80 percent. Ionic liquid forms deliver 85 to 95 percent. The form on your supplement label determines how much of the stated milligrams actually reaches your cells. [Full breakdown with absorption rate table in our Mineral Bioavailability post: link]
Never Miss any Updates From Blog!



No products in the cart.