Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
Up to 75 percent of women experience premenstrual symptoms. Bloating, breast tenderness, mood changes, fatigue, cramps, poor sleep. They arrive in the week or two before your period, and they leave when it begins.
PMS is not in your head. The symptoms are driven by specific hormonal and neurological changes in the luteal phase of your cycle, and each one has a mechanism that explains it.
What PMS does not have is a single cause. It involves the interaction of oestrogen and progesterone changes with serotonin, GABA, prostaglandins, and fluid regulation systems. That complexity is why there is no single treatment that resolves it for everyone, and why understanding which mechanism is driving your particular symptom picture matters for choosing what to try.
This post covers the mechanisms behind the most common PMS symptoms, what distinguishes PMS from PMDD, and what the research evidence actually says about relief.
BEFORE YOU READ FURTHER This post covers the mechanisms behind PMS symptoms and evidence-based approaches to relief. PMS is extremely common and for most women is manageable through lifestyle and nutritional approaches without requiring medical treatment. If your premenstrual symptoms are severe enough to significantly impair your daily function, relationships, or work across multiple cycles, you may be experiencing PMDD rather than PMS. PMDD is a distinct clinical condition that warrants assessment by your GP. This post covers PMS and includes a section explaining when the PMDD threshold may have been crossed. If your symptoms include thoughts of self-harm at any point in your cycle, please contact your GP or a crisis service. In Australia: Lifeline 13 11 14. |
DEFINITION PMS Premenstrual Syndrome. A pattern of physical and emotional symptoms that appear in the luteal phase of the menstrual cycle, typically in the one to two weeks before menstruation, and resolve within a few days of the period beginning. PMS is estimated to affect 20 to 40 percent of women of reproductive age to a degree that causes meaningful discomfort, with up to 75 percent experiencing some premenstrual symptoms. PMS is distinguished from the normal hormonal variation of the menstrual cycle by the consistency of the pattern and its impact on daily life. It is distinguished from PMDD by severity: PMS symptoms are uncomfortable but do not significantly impair daily function. The term ‘premenstrual tension’ (PMT) is an older name for the same condition, focused historically on its mood and tension components. The underlying cause is the interaction of normal luteal phase hormonal changes with serotonin, GABA, prostaglandin, and fluid-regulating systems. |
PMS symptoms span physical, emotional, and cognitive categories. Most women experience a consistent subset rather than the full range.
Physical symptoms: bloating and abdominal swelling; breast tenderness or soreness; headaches; joint or muscle aches; fatigue or low energy; sleep changes including insomnia or oversleeping; changes in appetite or food cravings; nausea; cramps before the period begins.
Mood and emotional symptoms: irritability or low frustration tolerance; anxiety or tension; low mood or tearfulness; mood swings; feeling overwhelmed.
Cognitive symptoms: difficulty concentrating; brain fog; forgetfulness.
The timing pattern is the diagnostic signal. Symptoms appear after ovulation, worsen in the week before menstruation, and resolve within one to two days of the period starting. If symptoms persist throughout the cycle or are absent in the premenstrual phase, PMS is less likely as a primary diagnosis.
DOES THIS APPLY TO YOU? If these symptoms are present and follow the luteal timing pattern, this is PMS. If symptoms are severe enough to prevent you from working, maintaining relationships, or functioning normally across most cycles, PMDD rather than severe PMS is the more clinically accurate framing and warrants GP assessment. The distinction matters because the evidence-based treatment approaches differ. |
One important note on timelines: any intervention for PMS should be assessed across two to three complete cycles before drawing conclusions. PMS symptoms vary in intensity between cycles naturally. A single cycle is not a reliable signal of whether something is working.
Understanding which symptoms you experience most consistently matters more than trying to address all of them. Different PMS symptoms have different primary drivers. Knowing the driver helps identify what is most likely to work.
PMS does not have a single cause. The symptom clusters trace to different biological pathways, all of which are triggered by the hormonal changes of the luteal phase. Understanding which pathway drives which symptom explains why different interventions work for different people.
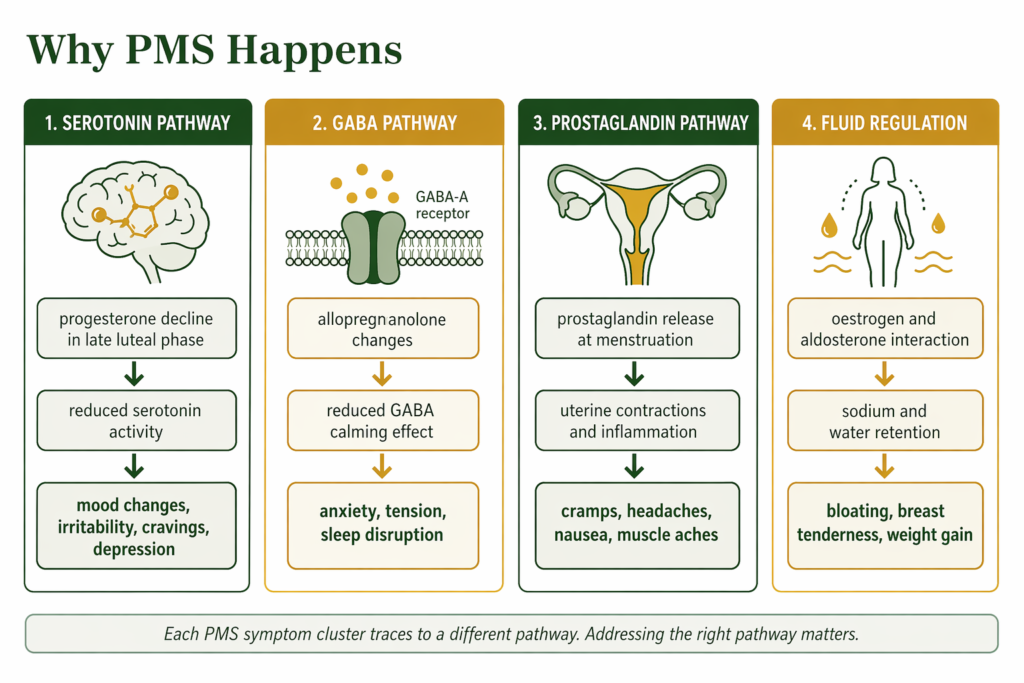
Oestrogen is associated with serotonin production and receptor sensitivity. In the luteal phase, as oestrogen fluctuates and progesterone rises then falls, serotonin activity may decrease. Research associates this change with the mood symptoms of PMS: irritability, low mood, tearfulness, and food cravings, particularly for carbohydrates, which are thought to temporarily support serotonin availability.
Progesterone is also associated with GABA-A receptor activity through its conversion to allopregnanolone, which is thought to have a calming effect. In the late luteal phase as progesterone drops, this effect may diminish, contributing to anxiety and tension alongside the serotonin-associated mood changes.
This dual pathway, serotonin and GABA, explains why the mood symptoms of PMS can include both low mood and anxiety simultaneously, and why the most effective pharmacological treatments for severe premenstrual mood symptoms work on these neurotransmitter systems.
Cramps and pain: at the start of menstruation, the endometrium releases prostaglandins, hormone-like compounds that trigger uterine contractions to shed the lining. Higher prostaglandin levels are associated with stronger contractions, more pain, and systemic symptoms including headaches, nausea, diarrhoea, and muscle aches. Women with greater sensitivity to prostaglandins tend to experience more severe cramping and physical symptoms.
Bloating and breast tenderness: oestrogen interacts with aldosterone, the hormone that regulates sodium and water balance, producing fluid retention in the luteal phase. This is primarily a hormonal response, though dietary factors such as high sodium intake may amplify it. The bloating and breast swelling typically resolve within a day or two of the period beginning regardless of dietary changes in the short term, which reflects the hormonal rather than purely nutritional driver.
Fatigue and sleep disruption: the decline in progesterone in the late luteal phase removes a sleep-promoting effect that progesterone provides through GABA receptor activity. Many women experience worse sleep quality, difficulty falling asleep, or early waking in the days before their period, independently of pain or other disruptive symptoms. The fatigue of PMS compounds when sleep quality is poor.
Food cravings: the serotonin drop in the late luteal phase drives carbohydrate cravings specifically, as carbohydrates temporarily increase brain tryptophan availability and serotonin production. This is a neurobiological response to serotonin depletion, not a lack of willpower.
DOES THIS APPLY TO YOU? If your PMS symptoms are predominantly physical, the prostaglandin and fluid regulation pathways are most likely primary. If they are predominantly mood-based, the serotonin and GABA pathways are more relevant. Most women experience a mix. The support section later in this post addresses both pathways, so you can identify which approaches are most relevant to your specific symptom pattern. |
The mechanism behind each symptom type maps directly to the interventions with the strongest evidence. This is why understanding the pathway matters before choosing what to try.
PMS and PMDD share timing and many surface symptoms. The distinction is severity and functional impact, not just the number of symptoms.
PMS is uncomfortable. Symptoms are present and noticeable but do not prevent you from working, maintaining relationships, or engaging with daily life. You may need to manage your schedule around your worst days, but you can function.
PMDD is functionally impairing. Mood symptoms, in particular, reach a severity that disrupts work, relationships, and sometimes safety. Women with PMDD describe being unable to be present in their lives during the luteal phase, not just uncomfortable in them.
The clinical distinction is not primarily about the type of symptoms but about their impact. Severe PMS that significantly impairs function meets the PMDD threshold. The treatment approaches also differ: for PMS, lifestyle and nutritional support are genuinely first-line. For PMDD, SSRIs are the most evidence-based primary treatment.
If your symptoms feel closer to the PMDD description, our dedicated post on PMDD symptoms and the neurobiological mechanism behind them covers the diagnostic criteria, clinical treatment options, and the specific brain mechanism that distinguishes PMDD from PMS.
DOES THIS APPLY TO YOU? If your premenstrual symptoms are uncomfortable but manageable, the approaches in this post are appropriate starting points. If they are significantly impairing your function, relationships, or safety across multiple cycles, GP assessment for PMDD is the right next step rather than trying to manage it as PMS. The interventions that work best for each condition differ substantially. |
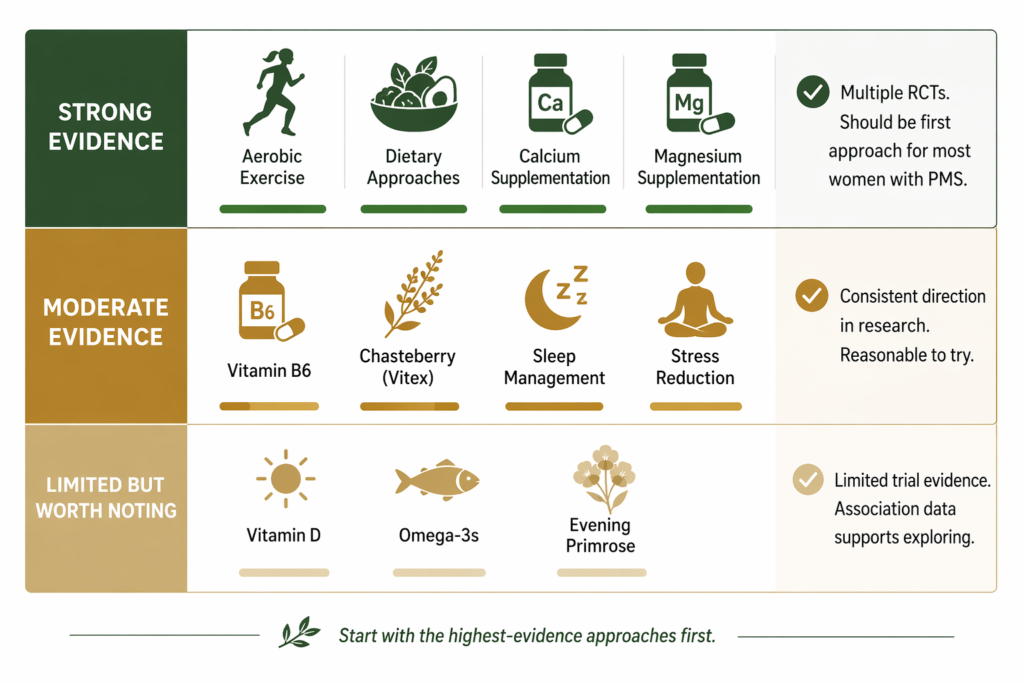
Aerobic exercise is one of the most consistently evidenced PMS interventions. Multiple studies have shown significant reductions in mood symptoms, bloating, and fatigue with regular moderate aerobic exercise. The mechanism includes serotonin and endorphin modulation directly addressing the neurobiological drivers of PMS mood symptoms. Three to five sessions of moderate aerobic activity per week shows the clearest benefit. Exercising regularly across the whole cycle, not just when symptomatic, produces better results than reactive exercise during symptoms.
Dietary pattern influences PMS through several mechanisms. Reducing refined carbohydrate and sugar intake stabilises blood glucose, preventing the cortisol spikes that amplify mood instability and worsen the already-compromised serotonin environment of the late luteal phase. High salt intake worsens fluid retention and bloating through the aldosterone pathway. Caffeine and alcohol in the luteal phase specifically increase neurological excitability and worsen sleep, amplifying both mood and physical symptoms. Adequate dietary protein supports serotonin precursor availability.
Sleep management in the luteal phase deserves specific attention rather than general sleep hygiene advice. Progesterone’s role as a GABA receptor agonist means its decline in late luteal phase specifically disrupts sleep architecture. Consistent sleep timing, cool sleeping environment, and avoiding alcohol in the luteal phase support the already-compromised sleep quality of this phase. A small amount of magnesium before bed may support GABA-related sleep calming during this period.
Stress reduction addresses PMS through the cortisol pathway. Elevated cortisol from sustained psychological stress places additional demand on the mineral reserves that support GABA and serotonin function, and adds neurological burden on top of the already-stressed luteal phase systems. This is not a generic recommendation: research consistently associates higher stress loads with worse PMS severity, and managing it is a targeted rather than general intervention. Ashwagandha has RCT evidence for reducing perceived stress and cortisol in stressed adults (Chandrasekhar et al., 2012). Its relevance to PMS is as a stress-load reducer, not as a direct hormonal or PMS treatment, and it is positioned here in that supportive capacity.
Several specific nutrients have been studied in randomised controlled trials for PMS. These are the strongest-evidenced options.
Calcium: among the most consistently evidenced supplements specifically for PMS. A large randomised controlled trial found significant reductions in overall PMS symptom scores, including mood symptoms, bloating, and pain, with supplementation at approximately 1,200mg per day (Thys-Jacobs et al., 1998). The effect size was clinically meaningful and the finding has been replicated. Calcium is involved in neurotransmitter signalling and is associated with GABA and serotonin pathway support. If you try one supplement for PMS, calcium has the strongest PMS-specific evidence.
Magnesium: multiple trials have shown reductions in mood symptoms, fluid retention, and pain with magnesium supplementation in PMS. Forms with higher bioavailability are generally preferred in research contexts. Magnesium supports GABA receptor function, which is directly relevant to the anxiety, tension, and sleep disruption of the late luteal phase. Taking magnesium before bed during the luteal phase specifically targets the GABA pathway during the period of greatest vulnerability.
Vitamin B6: evidence for reductions in mood symptoms at 50 to 100mg per day, through its role as a cofactor in serotonin and dopamine synthesis. Effect sizes are moderate but direction is consistent across multiple studies. Doses above 200mg per day have been associated with peripheral neuropathy and should be avoided.
Chasteberry (Vitex agnus-castus): has a number of trials showing reduction in PMS symptoms, particularly breast tenderness and mood symptoms. The mechanism is thought to involve dopamine receptor activity and indirect influence on prolactin, which contributes to breast tenderness and some mood symptoms. Evidence is moderate and some trials have methodological limitations, but it remains one of the more studied herbal options.
Magnesium is delivered alongside naturally occurring fulvic acid in Shilajit resin. For the context of why mineral form and delivery matters in practice, see our post on how mineral bioavailability affects what supplements actually do in the body.
For most women with PMS, lifestyle and nutritional approaches are sufficient and genuinely evidence-based first-line options. Medication is not automatically needed.
Non-prescription options: ibuprofen and naproxen are prostaglandin inhibitors and are effective for cramp and pain management. They address physical symptoms rather than the underlying hormonal mechanism but are appropriate for acute symptom management.
Prescription options: SSRIs are effective for mood-predominant PMS when lifestyle approaches are insufficient, and can be used only in the luteal phase rather than continuously. Combined oral contraceptives suppress ovulation and eliminate the hormonal fluctuation that drives PMS for some women. A GP can discuss which option fits your symptom pattern and history.
If you are starting from scratch, these are the three highest-leverage first steps based on the evidence above.
Step 1: Track your symptoms for two cycles before changing anything. Note which symptoms appear, when in your cycle they arrive, and their severity. This data is the foundation for knowing what to target and for any future GP conversation.
Step 2: Start aerobic exercise consistently if you are not already doing it. Three to five sessions of moderate activity per week across the whole cycle, not just when symptomatic, has the clearest evidence for mood and physical symptom reduction.
Step 3: Add calcium supplementation at around 1,200mg per day. This is the highest-evidence nutritional intervention for PMS across mood, physical, and bloating symptoms. Magnesium is a reasonable addition alongside it, particularly if sleep disruption and anxiety are prominent.
Your main PMS symptom | Evidence-based approaches to try first |
|---|---|
Mood swings and irritability | Regular aerobic exercise; calcium 1,200mg/day; magnesium supplementation; reduce caffeine and alcohol in luteal phase; blood glucose stability through reduced refined carbohydrates |
Low mood or tearfulness | Aerobic exercise (serotonin pathway); calcium 1,200mg/day; vitamin B6 50mg/day; consistent sleep timing in luteal phase |
Anxiety and tension | Magnesium before bed in luteal phase (GABA pathway); stress management; reduce caffeine; consistent sleep |
Cramps and physical pain | Ibuprofen or naproxen as needed; reduce saturated fat in luteal phase (reduces prostaglandin production); regular exercise across the cycle |
Bloating | Reduce sodium intake in luteal phase; reduce alcohol; consistent movement; note that this is primarily hormonal and fully resolves with the period regardless |
Breast tenderness | Reduce caffeine; chasteberry (Vitex) has moderate evidence; calcium 1,200mg/day |
Fatigue | Prioritise sleep quality in luteal phase; magnesium before bed; aerobic exercise (improves sleep quality and energy) |
Food cravings | Blood glucose stability through protein and fibre; note cravings are a neurobiological response to serotonin changes, not willpower failure |
WHAT TO DO ABOUT IT The most effective approach to PMS addresses the specific pathways driving your symptoms. For mood symptoms, serotonin support through regular aerobic exercise and blood glucose stability, alongside calcium and magnesium supplementation, targets the primary neurobiological drivers. For physical symptoms including cramping and pain, dietary reduction of saturated fat (which increases prostaglandin production) and ibuprofen or naproxen for acute pain management are appropriate first approaches. For bloating, reducing salt and alcohol in the luteal phase addresses the aldosterone-driven fluid retention. All of these are appropriate to try before considering pharmaceutical options, which are available if lifestyle and nutritional approaches are insufficient. |
DOES THIS APPLY TO YOU? If you have tried consistent lifestyle and nutritional approaches for two to three full cycles without adequate relief, GP assessment is the appropriate next step. This does not mean you have failed the self-management approach. It means you have useful evidence that your symptom severity may require additional support, which is clinically available and effective. |
Standard Thinking | The Biological Reality |
|---|---|
PMS is just hormones, you cannot do anything about it | PMS symptoms have specific neurobiological and physical mechanisms that respond to targeted interventions. Aerobic exercise, calcium, magnesium, dietary blood glucose stability, and sleep management all have meaningful trial evidence for PMS symptom reduction |
PMS mood symptoms are emotional, not physical | PMS mood changes are driven by serotonin and GABA system changes in the luteal phase. They are neurobiological, not psychological. The serotonin drop driven by oestrogen and progesterone changes is a physical event with a predictable emotional expression |
Bloating before your period means you are eating too much | Premenstrual bloating is driven by oestrogen and aldosterone-mediated fluid retention, not by food intake. It is hormonal, resolves independently of dietary changes, and disappears when the period begins regardless of what you eat |
PMS and PMDD are the same thing on a severity scale | They share timing and some symptoms but have different mechanisms and different evidence-based treatments. PMS involves normal sensitivity to hormonal changes. PMDD involves abnormal neurobiological sensitivity specifically to allopregnanolone fluctuation. This distinction determines which treatments are appropriate |
Calcium and magnesium supplements are a minor addition to PMS management | Calcium at 1,200mg per day has one of the strongest evidence bases of any supplement intervention in women’s health for PMS, with meaningful effect sizes in randomised controlled trials. Magnesium has consistent trial evidence for mood and fluid symptoms. They are not minor additions. They are among the most evidence-supported first-line options |
PMS symptoms fall into three categories. Physical symptoms include bloating, breast tenderness, cramps before the period, headaches, fatigue, changes in appetite, food cravings, nausea, and sleep disruption. Mood symptoms include irritability, low mood or tearfulness, anxiety, and mood swings. Cognitive symptoms include difficulty concentrating and brain fog. The defining pattern is that symptoms appear after ovulation in the luteal phase, typically in the week or two before menstruation, and resolve within a day or two of the period starting. If symptoms are present throughout the cycle rather than only in the luteal phase, another explanation is more likely.
PMS does not have a single cause. It results from the interaction of normal luteal phase hormonal changes with multiple biological systems. Serotonin activity decreases as oestrogen and progesterone fluctuate, driving mood symptoms and cravings. The GABA system is affected by changes in allopregnanolone, a progesterone metabolite, producing anxiety and sleep disruption. Prostaglandins released at menstruation drive cramping, pain, and systemic symptoms. Oestrogen interacts with aldosterone to produce fluid retention, bloating, and breast tenderness. Different women are more or less sensitive to each of these pathways, which is why PMS symptom patterns vary considerably between individuals.
The best-evidenced approaches for PMS are regular aerobic exercise, which modulates serotonin and reduces mood and physical symptoms; calcium supplementation at around 1,200mg per day, which has multiple randomised controlled trials showing meaningful symptom reduction; magnesium supplementation, which supports GABA function and reduces mood, fluid, and pain symptoms; and dietary approaches that reduce blood glucose instability, salt, caffeine, and alcohol in the luteal phase. Vitamin B6 has moderate evidence for mood symptoms. These lifestyle and nutritional approaches are genuinely first-line for most women with PMS and should be tried consistently across two to three cycles before considering pharmaceutical options.
No. PMS and PMDD share timing and some symptoms but are distinct conditions. PMS produces discomfort that does not significantly impair daily function. PMDD produces mood and cognitive symptoms severe enough to impair work, relationships, and sometimes safety. They also have different mechanisms: PMS involves normal sensitivity to the hormonal changes of the luteal phase, while PMDD involves an abnormal neurobiological response to allopregnanolone fluctuation specifically. The most effective treatments differ as a result. SSRIs are first-line for PMDD but not typically required for PMS. If your symptoms significantly impair your function, PMDD assessment is more appropriate than managing as severe PMS.
For some women PMS improves, for others it worsens as they move through their 30s and into perimenopause. Perimenopause, which typically begins in the mid-to-late 40s, can intensify PMS symptoms as hormonal fluctuation becomes more pronounced and progesterone production less consistent. Women with moderate PMS sometimes find it worsens significantly in their 40s and what they are experiencing has shifted toward a perimenopause-related hormonal picture. If your PMS has clearly worsened in your 40s alongside changes to your cycle, perimenopause is worth considering as a contributing factor and discussing with your GP.
ONE MORE THING BEFORE YOU GO If your PMS symptom pattern does not quite match what is described here, or if you are trying to work out whether what you experience is PMS, PMDD, or something else, leave it in the comments below. Tell us which symptoms are most prominent, when in your cycle they appear, and what you have already tried. We read every comment and respond with what the research says. If you have tried the lifestyle approaches and found limited relief, that is specifically useful information and we can help you think through what the next step might look like. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. PMDD is a clinical condition that requires assessment and management by qualified healthcare professionals. If you are experiencing symptoms consistent with PMDD, particularly if those symptoms include thoughts of self-harm, please seek appropriate clinical care promptly.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!



No products in the cart.