Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
It happens on schedule. Around the same point in your cycle, every month, something shifts. The mood drop comes first, or the rage, or a despair so heavy it does not feel proportionate to anything in your life. You are exhausted in a way that sleep does not fix. Your brain feels foggy. Your body aches.
And then your period arrives, and within a day or two, it is gone. You feel like yourself again.
That pattern, cyclical, predictable, tied to your luteal phase, is what distinguishes PMDD from primary depressive and anxiety disorders, though it can coexist with both. It is not extreme PMS. It is a specific neurobiological condition with a documented mechanism and established treatments that most women with PMDD never receive, often because diagnosis is delayed for years despite symptoms being present.
This post explains what PMDD actually is, what is happening in the brain during the luteal phase, how to distinguish it from PMS, and what the evidence says about treatment and support.
BEFORE YOU READ FURTHER PMDD is a recognised medical and psychiatric condition listed in the DSM-5 and ICD-11. It requires clinical diagnosis. This post is educational and intended to help you understand the mechanism and navigate the path to appropriate assessment and treatment. If you are experiencing thoughts of self-harm or suicide at any point in your cycle, please contact a crisis service or present to an emergency department immediately. PMDD is associated with elevated suicidality risk during the luteal phase. This is a medical emergency and not something to manage alone. In Australia: Lifeline 13 11 14. Beyond Blue 1300 22 4636. If your symptoms are severe, significantly affect your relationships or work, or you suspect PMDD, a GP referral to a gynaecologist or psychiatrist with PMDD experience is the appropriate first step. The information below will help you understand what you are describing and what to ask for. |
|
The diagnostic criteria for PMDD require five or more of the following symptoms, with at least one being a mood symptom, present in the luteal phase across most cycles for at least twelve months.
Mood symptoms (at least one required): marked mood swings, sudden sadness or tearfulness; persistent irritability or anger, often disproportionate to the situation; marked anxiety, tension, or feeling on edge; depressed mood, hopelessness, or self-critical thoughts.
Behavioural and cognitive symptoms: decreased interest in usual activities; difficulty concentrating; feeling overwhelmed, out of control, or unlike yourself; social withdrawal.
Physical symptoms: fatigue or low energy; changes in appetite, food cravings, or overeating; sleep disturbance; breast tenderness or swelling; headaches; joint or muscle aches; bloating or weight gain.
The critical diagnostic signal: all symptoms must resolve within a few days of menstruation beginning and be absent in the week after the period. If mood symptoms are present throughout the cycle, PMDD is less likely as a standalone diagnosis.
DOES THIS APPLY TO YOU? If this pattern matches your experience across multiple cycles, PMDD is a strong candidate diagnosis. Tracking your symptoms using a daily diary across two full cycles before your GP appointment is the most useful thing you can do. The International Association for Premenstrual Disorders (IAPMD) provides a validated tracking tool at iapmd.org. If symptoms are present throughout the cycle rather than only in the luteal phase, other conditions including clinical depression, anxiety, or ADHD may be primary and should be assessed alongside any PMDD investigation. |
Understanding the diagnostic pattern leads directly to the question most women ask next: why does this happen? The mechanism is specific and once you understand it, the treatment logic becomes clear.
PMDD is one of the most misunderstood conditions in women’s health because the cause appears to contradict the experience. Most women with PMDD have completely normal hormone levels.
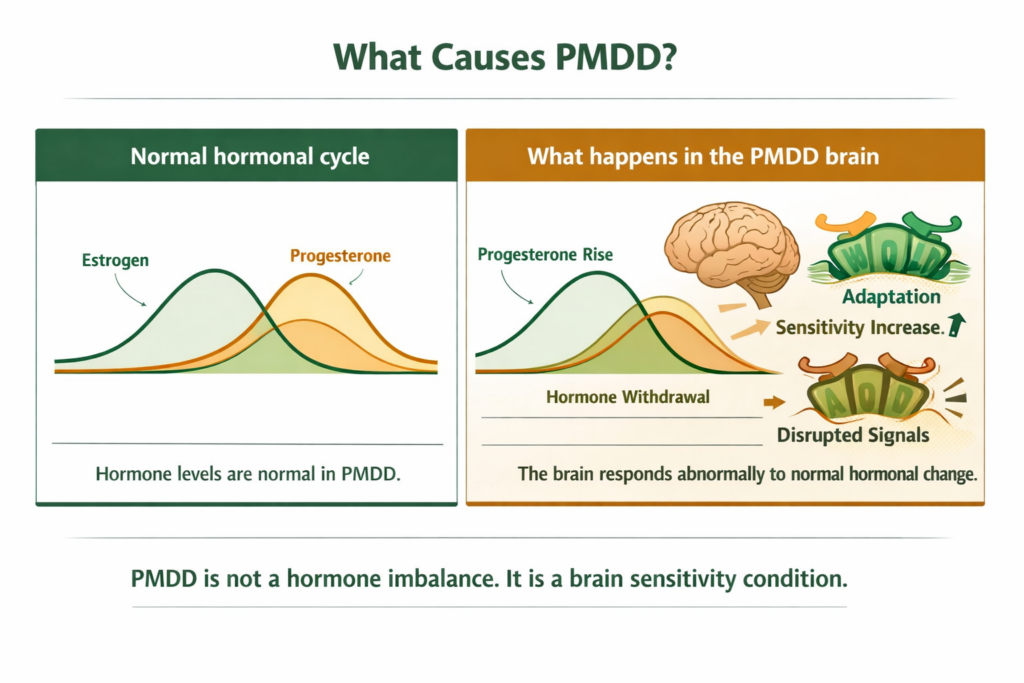
The mechanism: progesterone, once released after ovulation, is converted in the brain into a compound called allopregnanolone. Allopregnanolone acts on GABA-A receptors, the brain’s primary calming system. In most people, this interaction is calming and mood-stabilising during the luteal phase. In people with PMDD, the brain is abnormally sensitive to this fluctuation.
During the luteal phase, as allopregnanolone levels rise, the GABA-A receptors adapt by becoming less responsive. When allopregnanolone then drops sharply in the days before menstruation, the result is a withdrawal-like response in the nervous system. The GABA system is suddenly undersupported, and the brain responds with the characteristic PMDD symptom cluster: mood instability, anxiety, irritability, pain sensitivity, cognitive disruption, and fatigue.
This is not a psychological response to hormonal change. It is a neurobiological one. The brain is responding abnormally to a normal hormonal signal. Serotonin pathways are also affected: the allopregnanolone fluctuation disrupts the interaction between progesterone metabolites and serotonin receptor expression, which contributes to the depression and irritability symptoms and explains why serotonin-targeting medications are among the most effective treatments.
DEFINITION ALLOPREGNANOLONE A naturally occurring steroid produced in the brain from progesterone. It acts as a positive allosteric modulator of GABA-A receptors, meaning it enhances the calming, inhibitory effect of GABA in the brain. In healthy neurological function, allopregnanolone supports mood stability and reduces anxiety in the luteal phase. In PMDD, the brain adapts to the rising allopregnanolone of the luteal phase in a way that makes the subsequent pre-menstrual drop feel like a withdrawal. This withdrawal-like response to normal hormonal fluctuation is the central mechanism behind PMDD mood and anxiety symptoms. It explains why SSRI medications, which modulate serotonin and also influence GABA system sensitivity, are effective for PMDD. |
WHAT TO DO ABOUT IT Understanding that PMDD is a brain sensitivity condition, not a hormone excess or deficiency, is clinically important. Treatments that work address the brain’s response to hormonal change rather than the hormone levels themselves. This is why SSRIs are effective even when taken only in the luteal phase, and why hormonal contraceptives work for some women but not others. The goal of any approach is to reduce the severity of the GABA system’s response to the allopregnanolone shift, either by modulating that shift itself or by supporting the systems it disrupts. |
DOES THIS APPLY TO YOU? If you have had hormone level tests that came back normal and were told this rules out PMDD, that information is incorrect. Normal hormone levels are the expected finding in PMDD. The condition is diagnosed by symptom pattern across the cycle, not by blood tests. A normal oestrogen or progesterone result does not rule out PMDD. |
The mechanism explains the treatment hierarchy. What works for PMDD works specifically on the neurobiological response to hormonal change, not on the hormones themselves.
PMS and PMDD share timing and some symptom overlap, but they are not the same condition on a severity spectrum. They differ in the nature and impact of symptoms.
PMS produces physical symptoms including bloating, breast tenderness, and fatigue, alongside mild mood changes. Symptoms are present but do not significantly impair daily function. Most women with PMS can work, maintain relationships, and engage normally with daily life during the premenstrual phase, even if uncomfortably.
PMDD involves mood and cognitive symptoms of a severity that impairs function. The depression, rage, anxiety, or despair of PMDD is not mild premenstrual moodiness. It is disruptive. Women with PMDD report being unable to work, damaging relationships, withdrawing from social contact, and experiencing thoughts of self-harm during the luteal phase. The functional impairment is the clinical distinction, not just symptom severity alone.
The overlap zone matters because many women are diagnosed with severe PMS when they actually meet criteria for PMDD. If your premenstrual symptoms significantly disrupt your life, relationships, or work across multiple cycles, PMDD rather than PMS is the more clinically accurate framing, and the treatment approach is different.
Perimenopause can intensify PMDD or produce a PMDD-like picture in women who did not previously have it. As progesterone production becomes less consistent, the sensitivity-withdrawal cycle can become more pronounced. For the full perimenopause context, see our post on perimenopause symptoms and the hormonal mechanisms behind the transition.
DOES THIS APPLY TO YOU? If your premenstrual symptoms are uncomfortable but manageable, general PMS support measures including lifestyle approaches and nutritional support may be sufficient. If your symptoms are severe enough to affect your function, relationships, or safety, PMDD is the appropriate framing and clinical assessment is necessary. The distinction matters because the treatment options differ significantly. |
PMDD is diagnosed clinically through prospective symptom tracking, not through blood tests. Hormone levels are typically normal and a normal result does not rule out the condition.
The standard diagnostic approach involves keeping a daily symptom diary across two complete menstrual cycles. The diary records the presence and severity of mood, cognitive, and physical symptoms each day. The pattern that confirms PMDD is symptoms present and functionally impairing in the luteal phase, resolving within days of the period starting, and absent in the week following menstruation.
Validated tools: the Daily Record of Severity of Problems (DRSP) and the Carolina Premenstrual Assessment Scoring System (C-PASS) are validated instruments used in clinical practice. The IAPMD (iapmd.org) provides accessible tracking resources and guidance on how to present your symptom history to a clinician.
Who to see: your GP is the appropriate first contact. They can exclude other conditions, refer to a gynaecologist or psychiatrist with PMDD experience, and initiate first-line treatment. If your GP is not familiar with PMDD, IAPMD’s clinician directory can help identify a specialist.
DOES THIS APPLY TO YOU? If you suspect PMDD, begin tracking your symptoms daily before your GP appointment. A two-cycle diary is more diagnostically useful than a retrospective account of how you feel. Note the timing of symptoms relative to your cycle, their severity on a 1 to 10 scale, and their functional impact. This evidence significantly improves the likelihood of an accurate and timely diagnosis. |
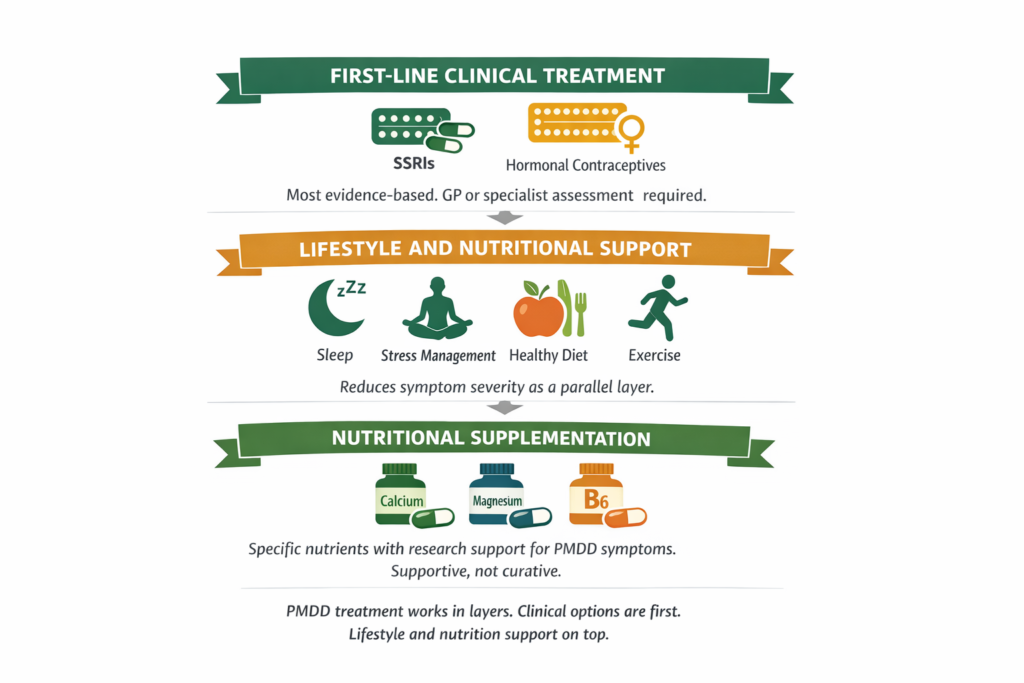
SSRIs are the most evidence-based pharmacological treatment for PMDD and are specifically approved for this indication. Unlike their use in depression, SSRIs for PMDD can be taken continuously or only during the luteal phase, typically from ovulation until the start of menstruation. Luteal-phase dosing is effective for many women and reduces side effects associated with continuous use. Common SSRIs used include fluoxetine, sertraline, and paroxetine. Response rates in clinical trials are high, often 60 to 70 percent reporting significant symptom reduction.
Hormonal contraceptives work for some women with PMDD by suppressing ovulation and therefore eliminating the hormonal fluctuation that triggers the allopregnanolone sensitivity response. The combined oral contraceptive containing drospirenone and ethinylestradiol has the most evidence for PMDD specifically. Hormonal approaches do not work for all women with PMDD and can worsen symptoms in some cases.
In severe or treatment-resistant PMDD, GnRH agonists, which suppress ovarian function entirely, are used under specialist supervision. Surgical options are considered in the most refractory cases.
Your GP can initiate SSRI treatment and discuss contraceptive options. For more complex presentations, the Jean Hailes for Women’s Health resource at jeanhailes.org.au and the IAPMD at iapmd.org both provide clinician directories and evidence-based guidance.
Lifestyle approaches reduce the severity of PMDD symptoms and improve response to clinical treatment. They do not replace clinical treatment in significant PMDD.
Aerobic exercise has consistent evidence for reducing mood and physical symptoms in PMS and PMDD. The mechanism includes serotonin and GABA modulation, which directly addresses the neurobiological pathway underlying PMDD. Three to five sessions of moderate aerobic activity per week is the most supported approach.
Sleep disruption amplifies PMDD severity. During the luteal phase the circadian rhythm is affected by progesterone, making sleep less restorative. Prioritising sleep quality during the luteal phase specifically, rather than treating it as a standard every-night concern, is a targeted and practical approach.
Dietary pattern influences PMDD through multiple pathways. Reducing refined carbohydrate intake stabilises blood glucose, which reduces cortisol spikes that amplify mood instability. Adequate dietary protein supports serotonin precursor availability. Reducing caffeine and alcohol in the luteal phase specifically reduces neurological excitability during the period of greatest vulnerability.
Stress load amplifies PMDD severity. High sustained psychological stress increases cortisol, which places additional demand on the neurological systems already stressed by the allopregnanolone withdrawal response. Managing stress is not a generic recommendation here: it is a specific intervention with a specific mechanism.
Several specific nutrients have been studied in randomised controlled trials for PMS and PMDD. These are the strongest-evidenced options in the supplementation category.
Calcium: multiple randomised controlled trials have demonstrated significant reductions in mood and physical PMDD symptoms with calcium supplementation at around 1,200mg per day. The effect size is meaningful and the evidence is more robust than for most other supplements studied in this context. The mechanism is thought to involve calcium’s role in neurotransmitter signalling, including in the GABA pathway (Thys-Jacobs et al., 1998).
Magnesium: research associates magnesium status with PMS and PMDD symptom severity. Several trials have shown reductions in mood symptoms, fluid retention, and pain with magnesium supplementation. Forms with higher bioavailability are generally preferred in research contexts. The mechanism includes magnesium’s support of GABA receptor function and its role in regulating neurological excitability during hormonal transitions.
Vitamin B6: has evidence for reducing mood symptoms in PMS at doses of 50 to 100mg per day, likely through its role as a cofactor in serotonin and dopamine synthesis. Evidence is more moderate than for calcium but consistent in direction.
Lower vitamin D status is associated with greater PMDD severity in observational research, though supplementation trial evidence is limited. Addressing deficiency through a GP if relevant is reasonable but vitamin D is not a primary PMDD intervention.
Magnesium’s role in GABA receptor support is specifically relevant in PMDD given that the core mechanism involves GABA-A receptor sensitivity to allopregnanolone withdrawal. Forms with higher bioavailability are generally preferred in research contexts. The broader context of how different mineral forms compare is covered in our post on how mineral bioavailability affects what supplements actually do in the body.
WHAT TO DO ABOUT IT The evidence-based approach to PMDD works in order. Clinical assessment and treatment comes first for significant PMDD: SSRI treatment and hormonal options have the strongest evidence and the highest effect sizes. Lifestyle foundations including aerobic exercise, sleep quality in the luteal phase, dietary blood glucose stability, and stress load reduction support clinical treatment. Nutritional supplementation, particularly calcium and magnesium, has meaningful supporting evidence and is appropriate as a parallel layer. Symptom tracking across two cycles before your GP appointment is the most useful single action if you have not yet sought diagnosis. |
DOES THIS APPLY TO YOU? If your PMDD symptoms are severe, involve thoughts of self-harm, or are significantly affecting your daily function, clinical treatment is the appropriate primary response. Lifestyle and supplement approaches are relevant as supportive layers alongside clinical treatment, not as replacements for it. If you have already tried lifestyle approaches without adequate relief, that is specifically the information to bring to your GP to support moving toward pharmaceutical options. |
If you are building the nutritional and lifestyle foundation alongside clinical assessment, magnesium and stress management are the two areas with the most direct relevance to the neurobiological mechanisms described above.
Standard Thinking | The Biological Reality |
|---|---|
PMDD is just bad PMS | PMDD is a distinct clinical diagnosis with different diagnostic criteria and different treatment options from PMS. The functional impairment is the clinical distinction. Severe premenstrual symptoms that affect your ability to work, maintain relationships, or stay safe are PMDD territory, not PMS |
Normal hormone tests rule out PMDD | PMDD is caused by abnormal sensitivity to normal hormonal changes, not by abnormal hormone levels. Normal oestrogen and progesterone results are the expected finding in PMDD. Diagnosis is based on symptom pattern across the cycle, not on blood test results |
PMDD is a mental health problem | PMDD is a neurobiological condition with a documented mechanism involving GABA-A receptor sensitivity to allopregnanolone fluctuation. It is listed in the DSM-5 as a mental health condition and in the ICD-11 as a gynaecological one. Both are accurate. The distinction matters less than accessing appropriate treatment |
You just need to manage your stress | Stress amplifies PMDD severity through the cortisol pathway but does not cause it. The core mechanism is the brain’s response to allopregnanolone withdrawal. Managing stress is a supportive intervention. It does not address the primary neurobiological condition |
Supplements can treat PMDD | Calcium and magnesium have research support for reducing PMDD symptom severity. They are not treatments for the condition. SSRIs and hormonal approaches have far stronger evidence and effect sizes for significant PMDD. Supplements belong in the supportive layer, not the primary treatment position |
PMDD (Premenstrual Dysphoric Disorder) is a recognised psychiatric and gynaecological condition in which severe mood, cognitive, and physical symptoms appear in the luteal phase of the menstrual cycle, typically in the one to two weeks before menstruation, and resolve within days of the period beginning. It is distinct from PMS in its severity and its functional impact. PMDD affects approximately 3 to 8 percent of women of reproductive age. It is caused not by abnormal hormone levels but by abnormal neurobiological sensitivity to the normal hormonal changes of the luteal phase, specifically the brain’s response to fluctuating allopregnanolone, a progesterone metabolite that acts on GABA-A receptors.
PMDD symptoms include at least one mood symptom from: marked mood swings, sudden tearfulness, persistent irritability or anger, and marked anxiety or tension. Additional symptoms can include depressed mood or hopelessness, decreased interest in usual activities, difficulty concentrating, fatigue, changes in appetite or sleep, physical symptoms including bloating, breast tenderness, and headaches, and a feeling of being overwhelmed or out of control. The defining feature is that all symptoms appear in the luteal phase and resolve within a few days of menstruation beginning. Symptoms are severe enough to impair daily function, relationships, and work.
PMS and PMDD share timing but differ in severity and functional impact. PMS produces physical symptoms and mild mood changes that are uncomfortable but do not significantly impair daily function. PMDD involves mood and cognitive symptoms of a severity that disrupts work, relationships, and safety. Women with PMDD may be unable to function normally during the luteal phase. The diagnostic threshold for PMDD requires five or more specified symptoms with at least one mood symptom, present across most cycles for at least twelve months, causing significant functional impairment. If your premenstrual symptoms affect your ability to function, PMDD is the more clinically accurate framing.
The most evidence-based treatments for PMDD are SSRIs (selective serotonin reuptake inhibitors), which can be taken continuously or only in the luteal phase, and certain hormonal contraceptives, particularly those containing drospirenone. SSRIs show response rates of 60 to 70 percent in clinical trials and are specifically approved for PMDD. Lifestyle approaches including regular aerobic exercise, sleep quality management, and dietary blood glucose stability support clinical treatment. Nutritional supplementation, particularly calcium at around 1,200mg per day, has meaningful trial evidence for symptom reduction. GP assessment is the appropriate starting point for accessing effective treatment.
PMDD can intensify during perimenopause, the transition phase before menopause. As progesterone production becomes less regular and ovulation less consistent, the hormonal fluctuations that trigger the allopregnanolone sensitivity response can become more unpredictable. Women who had mild or manageable PMDD in their 30s sometimes find it significantly worsens in their 40s. In some women, perimenopause can produce a PMDD-like picture for the first time. If your premenstrual symptoms are worsening in your 40s, perimenopause may be a contributing factor and is worth raising with your GP.
ONE MORE THING BEFORE YOU GO If your symptom pattern does not quite match what is described here, or if you are trying to work out whether what you experience is PMDD, severe PMS, or something else entirely, leave it in the comments. Tell us what your cycle looks like, when symptoms arrive, and when they leave. We read every comment and respond with what the research says about your specific pattern. If you have already been dismissed by a GP or told your hormone tests were normal and therefore nothing is wrong, that is specifically the experience we can help you understand and navigate. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. PMDD is a clinical condition that requires assessment and management by qualified healthcare professionals. If you are experiencing symptoms consistent with PMDD, particularly if those symptoms include thoughts of self-harm, please seek appropriate clinical care promptly.

Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!Never Miss any Updates From Blog!
Never Miss any Updates From Blog!



No products in the cart.