Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
Your muscles are cramping. Not just during exercise. At rest, at night, without obvious reason. You feel weaker than you should. Tired in a way that does not quite match your sleep. Your heart occasionally flutters or races when it has no reason to.
These symptoms can share a common underlying cause. They are worth investigating together rather than as separate problems.
Potassium plays a central role in the electrical charge across cell membranes. Muscle contraction, nerve signalling, and cardiac rhythm all depend on potassium moving in and out of cells to generate and reset that charge. When potassium is consistently low, these processes can become disrupted in ways that produce cramps, weakness, palpitations, and fatigue. The mechanism is well-documented, though the symptoms are non-specific and share overlap with other mineral deficiencies and causes.
This post explains the mechanism, how to distinguish the potassium pattern from other common causes, and what the evidence says about restoration.
BEFORE YOU READ FURTHER This post covers the symptoms and mechanisms of potassium deficiency. These are real, well-documented biological effects of low potassium status. If you are experiencing severe muscle weakness, difficulty breathing, an irregular heartbeat that is new or has worsened recently, or if you are on medications including diuretics, ACE inhibitors, or digoxin, please see a GP before attempting to self-manage potassium levels. Potassium interacts with several common medications and severe deficiency requires clinical monitoring. If you are experiencing the gradual symptom pattern described here, particularly muscle cramps, persistent weakness, fatigue, and sleep disruption, and you have a diet low in vegetables and whole foods, this post is written for your situation. |
Mark the ones that apply consistently over the past few weeks.
Muscle cramps, particularly in the legs. Cramping at rest or at night, not only during exercise. Calves, feet, or thighs most commonly.
General muscle weakness. Muscles that feel heavier or less responsive than usual. Physical tasks that seem disproportionately difficult.
Persistent fatigue. Low energy that does not fully resolve with sleep or rest.
Constipation or sluggish digestion. Slower than usual, without a dietary change that explains it.
Heart palpitations. Awareness of an irregular or faster heartbeat, particularly at rest.
Muscle twitching. Small involuntary muscle contractions, often in the legs, eyelids, or hands.
Numbness or tingling. Particularly in the hands, feet, or face. A pins-and-needles quality without a positional cause.
Difficulty sleeping. Restlessness, leg discomfort at night, or waking feeling unrestored.
If three or more of these are consistently present, particularly if muscle cramps and fatigue are both in the picture, low potassium is worth investigating. The sections below explain the mechanism and how to distinguish the potassium pattern from other common causes. If the pattern fits, the final section covers how to confirm and address it.
Note: these symptoms overlap significantly with magnesium deficiency and dehydration. The presence of multiple symptoms together, particularly cramps alongside weakness and digestive changes, is more informative than any single symptom alone.
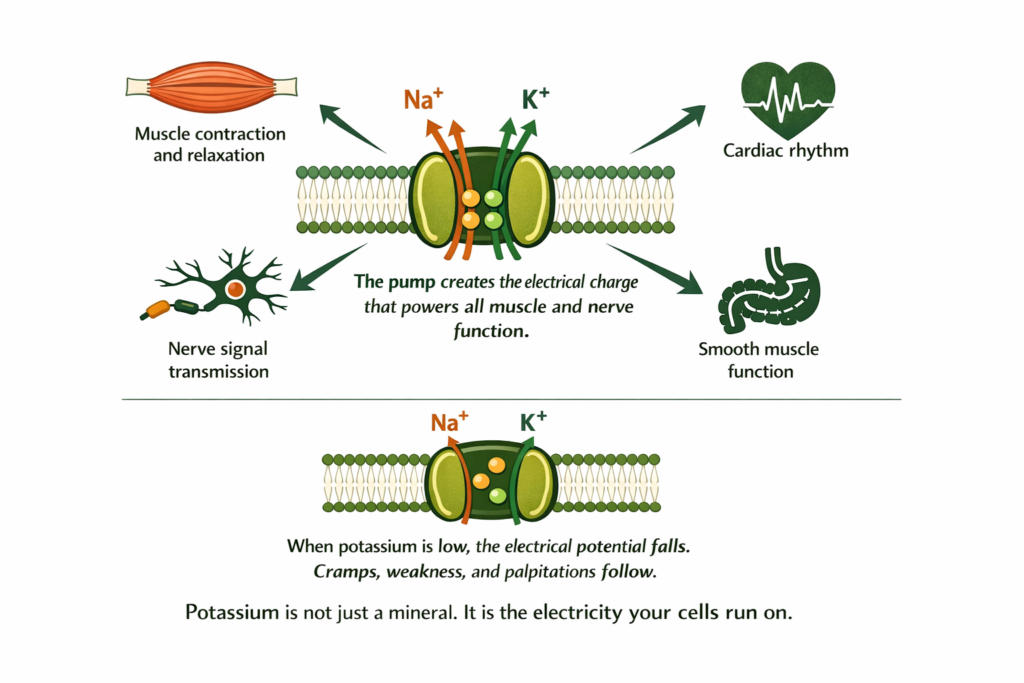
Every cell in your body maintains an electrical charge across its membrane. The inside of the cell is negatively charged relative to the outside. This charge is what allows muscles to contract, nerves to fire, and the heart to beat in rhythm.
This electrical charge is maintained by the sodium-potassium pump: a protein engine embedded in every cell membrane that continuously moves potassium into cells and sodium out, at a ratio of two potassium in for every three sodium out. This pump consumes approximately 25 to 40 percent of the body’s total energy production. It runs continuously, every second of every day, including throughout sleep.
When potassium is insufficient, the pump cannot maintain the electrical charge. The membrane potential falls. Muscles cannot contract and relax properly, which is associated with cramps, weakness, and twitching. Cardiac electrical conduction can become less stable, which is associated with palpitations and rhythm disturbances. Nerve signalling and smooth muscle function are also affected (Gennari, 1998). The potassium deficiency symptom cluster is well-documented in clinical literature, though the severity of symptoms varies considerably between individuals and not all people with low serum potassium experience symptoms.
DEFINITION SODIUM-POTASSIUM PUMP A protein channel embedded in every cell membrane that actively moves potassium ions into cells and sodium ions out, against their natural concentration gradients. This process creates and maintains the electrical potential across the cell membrane that powers all muscle contraction, nerve signalling, and cardiac rhythm. The pump requires constant energy, consuming a large portion of the body’s ATP. When potassium is low, the pump cannot maintain adequate cellular potassium levels and the electrical potential falls. Restoring potassium through diet or supplementation provides the raw material the pump needs to re-establish the charge. |
Recommended intake for context: Adults require 2,600mg of potassium per day (women) to 3,400mg (men) according to dietary reference intakes (Institute of Medicine, 2005). Most people consuming a diet low in vegetables, legumes, and whole foods fall short of this. A medium banana provides approximately 422mg. A cup of cooked spinach provides approximately 840mg. Consistent dietary gaps over weeks to months are the most common cause of the low-potassium symptom pattern described below.
Each symptom below is associated with low potassium based on the cellular mechanism above. The sections note where other causes produce similar patterns.
Muscle contraction requires a rapid change in membrane potential: the cell depolarises, the muscle fibre contracts, then the membrane potential is restored and the muscle relaxes. This sequence depends on adequate potassium to reset the membrane after each contraction.
When potassium is low, the muscle cannot fully relax between contractions. The depolarisation happens but the repolarisation is incomplete. The muscle stays in a partially contracted state. This is what a cramp is: a sustained involuntary contraction that the muscle cannot release because the electrical reset mechanism does not have the potassium it needs.
Weakness follows from the same mechanism. When the electrical potential is chronically low, the muscle cannot generate its full contractile force. Tasks that should be easy require disproportionate effort. The weakness often has a heavy quality: muscles that feel leaden rather than painful.
Cramps at night are particularly common because the body’s potassium regulation changes during sleep, and the low-potassium state becomes more apparent when muscle activity drops but the resting electrical requirement remains.
WHAT TO DO ABOUT IT Muscle cramps from low potassium respond to dietary potassium restoration in the short term and to addressing the pattern that caused the depletion in the longer term. High-potassium foods including bananas, avocados, leafy greens, potatoes, and legumes should form the foundation. For immediate cramp relief, ionic potassium alongside ionic magnesium addresses both the electrical and the muscle relaxation deficits simultaneously. Magnesium is required for the sodium-potassium pump to function and the two deficiencies frequently occur together. |
DOES THIS APPLY TO YOU? If muscle cramps are exclusively during or immediately after intense exercise and resolve quickly with rest and rehydration, dehydration and acute electrolyte loss is the more likely cause. Potassium-related cramps typically occur at rest, at night, or with minimal activity, and are accompanied by the weakness and fatigue pattern described above. Dehydration cramps tend to be isolated. Potassium-pattern cramps tend to recur as part of a broader symptom picture. |
The heart is a muscle. It contracts and relaxes with every beat, governed by its own electrical conduction system. That system is acutely sensitive to potassium levels.
When potassium is low, cardiac cells become hyperexcitable. The membrane potential is unstable, and the electrical signals that normally produce a regular, coordinated heartbeat become irregular. The result is palpitations: the awareness of an unusual heartbeat, a flutter, a racing sensation, or skipped beats. In people with significant potassium deficiency, electrocardiogram changes are measurable.
Blood pressure is also affected. Potassium helps relax the walls of blood vessels and reduces the cardiovascular system’s response to sodium. Low potassium allows sodium’s blood-pressure-raising effects to operate without counterbalance, contributing to elevated blood pressure particularly in people who also have high sodium intake.
DOES THIS APPLY TO YOU? Palpitations have multiple causes and cardiac conditions must be excluded before attributing them to mineral deficiency. If palpitations are new, frequent, severe, accompanied by chest pain, breathlessness, or dizziness, or if you are over 40 with no prior cardiac assessment, see a GP and request an ECG first. Potassium-related palpitations are typically mild and improve alongside the broader symptom cluster as potassium is restored. They do not occur in isolation. |
Fatigue from low potassium is distinct from iron-deficiency fatigue. It has a heavy, muscular quality. The body feels physically difficult to move. This is because energy production itself depends on the sodium-potassium pump running efficiently. The pump uses ATP. When potassium is low and the pump is working inefficiently, cellular energy metabolism is disrupted and the body produces less usable energy per unit of fuel consumed.
Constipation from low potassium follows the same muscle weakness mechanism applied to the smooth muscle of the digestive tract. Peristalsis, the wave-like muscle contractions that move food through the intestines, weakens when potassium is insufficient. Digestion slows. Constipation arrives gradually and is often attributed to diet or stress rather than to mineral status.
Sleep disruption in low potassium presents differently from the sleep anxiety pattern or the 3am cortisol pattern. It tends to involve restlessness, leg discomfort at night, and a sense of physical unease that prevents settling rather than the mental activation of cortisol-driven sleeplessness. The muscle cramping and the lower-grade electrical instability in peripheral nerves makes the body feel uncomfortable at rest.
WHAT TO DO ABOUT IT Addressing the full symptom cluster requires consistent potassium restoration over two to four weeks before the full improvement becomes apparent. Energy and digestion typically respond faster than muscle cramps. Sleep disruption related to nighttime leg discomfort often improves within one to two weeks of restoring potassium and magnesium simultaneously, since magnesium is required for both muscle relaxation and the pump function that potassium depends on. |
This is the section most people with persistent low-potassium symptoms need to read, because restoring potassium alone often produces only partial improvement.
Magnesium is an essential cofactor for the sodium-potassium pump. The pump requires magnesium to function correctly. Without adequate magnesium, the pump cannot maintain cellular potassium levels even when dietary potassium is adequate. The potassium leaks out of cells regardless of how much you consume. This is called refractory hypokalaemia: low cellular potassium that does not respond to potassium supplementation because the underlying magnesium deficit has not been addressed.
The two deficiencies share common causes. Chronic stress depletes both. Diuretics cause urinary loss of both. Alcohol consumption depletes both. Diets low in vegetables and whole foods are insufficient for both. When potassium is low, magnesium is almost always low as well, and the two need to be restored in parallel.
For those looking at supplemental options beyond standard glycinate or citrate forms, Shilajit resin delivers potassium, magnesium, and over 80 trace minerals in their ionic forms alongside fulvic acid. The fulvic acid transport mechanism is the relevant distinction: it supports cellular mineral uptake alongside dietary and standard supplementation approaches. This is one option among several for addressing the co-depletion pattern.
Whichever approach is used, the evidence base for addressing both potassium and magnesium together is well-established in the context of refractory hypokalaemia, where magnesium repletion is required for potassium retention to succeed (Huang and Kuo, 2007).
Why the sodium-potassium pump depends on magnesium and why the form of mineral delivery determines whether it reaches the intracellular level is covered in our post on mineral bioavailability and why the form determines whether minerals reach your cells.
The magnesium side of the co-depletion pattern and what low magnesium specifically produces is covered in our post on symptoms of magnesium deficiency and the mechanism behind each one.
WHAT TO DO ABOUT IT Restore both potassium and magnesium simultaneously. The foundation is dietary: leafy greens, avocados, potatoes, bananas, and legumes for potassium; nuts, seeds, and dark chocolate for magnesium. Standard magnesium glycinate or citrate supplements are well-absorbed options for supplemental magnesium. For those who want to address the broader ionic mineral picture including the trace cofactors that support the sodium-potassium pump, ionic mineral delivery via fulvic acid is one approach that addresses multiple mineral gaps simultaneously. The most important step is consistency across both minerals over several weeks, whichever approach is used. |
DOES THIS APPLY TO YOU? If you have tried increasing dietary potassium through food and noticed limited improvement in cramps and weakness, the magnesium co-depletion is almost certainly the reason. The pump cannot hold cellular potassium without magnesium regardless of how much potassium you consume. If you are on prescribed diuretics or other medications that affect potassium, discuss supplementation with your GP before increasing potassium intake significantly. |
Understanding what depleted your potassium in the first place determines whether the restoration holds.
Diet low in vegetables and whole foods is the most common cause. The richest potassium sources are leafy greens, legumes, potatoes, avocados, bananas, and squash. Diets heavy in processed foods provide almost no potassium because processing removes it.
Chronic stress and sustained cortisol elevation increase urinary potassium loss. The same HPA axis activation pattern that depletes magnesium also accelerates potassium excretion through the kidneys.
High sodium intake drives more potassium out through the kidneys. The body maintains a sodium-potassium balance and excess sodium tips it toward potassium loss.
Diuretics and certain medications including some blood pressure medications, laxatives used long-term, and some antifungals can cause significant potassium loss. This is why potassium levels are monitored in people on these medications.
Alcohol increases urinary potassium excretion and typically accompanies dietary patterns low in potassium-rich foods.
Excessive sweating from intense exercise or heat causes electrolyte loss including potassium. Athletes with heavy training loads and high sweat rates are at particular risk if electrolyte replacement is insufficient.
Standard Thinking | The Biological Reality |
|---|---|
Muscle cramps are from dehydration or overexertion | Muscle cramps at rest and at night are most commonly from electrolyte deficiency rather than dehydration alone. Potassium and magnesium depletion both prevent proper muscle relaxation after contraction. Hydration alone does not restore them |
Eat more bananas for potassium | Bananas are a useful source but a single banana provides approximately 422mg of potassium against a daily requirement of 2,600 to 3,400mg. Dietary restoration requires consistently potassium-rich eating across the whole diet, not a single food |
Potassium supplements are all the same | The form and delivery mechanism determine how much potassium reaches cells. Additionally, potassium supplements without addressing concurrent magnesium deficiency often fail because the sodium-potassium pump cannot retain cellular potassium without adequate magnesium |
If potassium is low my doctor would have found it | Standard blood tests measure serum potassium, which the body tightly regulates. Intracellular potassium can be depleted while serum potassium remains in the normal range. Symptoms often precede serum changes |
What are the signs of low potassium?
The most consistent signs of low potassium are muscle cramps particularly at rest or at night, general muscle weakness with a heavy or leaden quality, persistent fatigue that has a physical rather than purely mental character, heart palpitations or awareness of an irregular heartbeat, constipation without a dietary change that explains it, muscle twitching, numbness or tingling especially in the extremities, and difficulty sleeping due to physical restlessness or leg discomfort. These symptoms all trace to the disrupted cellular electrical potential that potassium maintains through the sodium-potassium pump.
Why does low potassium cause muscle cramps?
Muscle contraction requires a rapid change in cellular electrical potential: the cell depolarises to contract and then repolarises to relax. Potassium is required for the repolarisation step. When potassium is insufficient, the membrane cannot fully reset after contraction. The muscle stays in a partially contracted state. This is the mechanism of a cramp: a sustained involuntary contraction the muscle cannot release because the electrical reset mechanism lacks the potassium it needs. Cramps at night occur because the low-potassium state becomes more apparent when voluntary muscle activity stops but the resting electrical requirement remains.
Can low potassium cause heart palpitations?
Yes, through the cardiac electrical conduction mechanism. The heart’s electrical system depends on stable cellular potassium levels to produce regular, coordinated beats. When potassium is low, cardiac cells become hyperexcitable and the membrane potential becomes unstable, producing irregular firing patterns experienced as palpitations, flutter, or racing. Blood pressure is also affected because potassium helps relax blood vessel walls and counterbalances sodium. Mild palpitations alongside other low potassium symptoms are typically the potassium mechanism. Frequent or severe palpitations, particularly in combination with chest pain or breathlessness, warrant GP assessment and an ECG.
Why doesn’t just eating more potassium fix the cramps?
Because potassium retention in cells depends on magnesium. The sodium-potassium pump, which maintains cellular potassium levels, requires magnesium to function correctly. Without adequate magnesium, the pump cannot retain potassium in cells regardless of how much is consumed. This is why potassium alone often produces only partial improvement while potassium and magnesium restored together produces more complete resolution. The two deficiencies share common causes and almost always occur together, so both need to be addressed simultaneously.
How long does it take to recover from low potassium?
With consistent dietary restoration and supplementation, energy levels and constipation typically improve within one to two weeks. Muscle cramps often improve within two to three weeks when both potassium and magnesium are addressed simultaneously. Heart palpitations related to potassium typically improve alongside the muscle and energy improvements over two to four weeks. Full recovery of cellular potassium stores, which requires both adequate dietary intake and restored magnesium pump function, typically takes four to six weeks of consistent approach. If symptoms do not meaningfully improve within four weeks, GP assessment and serum electrolyte testing is the appropriate next step.
Can low potassium cause anxiety?
Low potassium is not a primary cause of anxiety. However, because potassium affects nerve excitability and cardiac rhythm, some people with low potassium experience physical sensations such as palpitations, muscle twitching, and general unease that can be interpreted as or accompany anxiety. If anxiety is a primary symptom, magnesium deficiency, vitamin D insufficiency, thyroid dysfunction, and cortisol dysregulation are more common drivers and should be assessed first. Potassium is worth including in a broader mineral assessment but is not a standalone explanation for anxiety.
What foods fix potassium deficiency fast?
The highest dietary potassium sources are cooked spinach at approximately 840mg per cup, baked potato with skin at approximately 925mg, avocado at approximately 690mg per half, cooked lentils at approximately 730mg per cup, and banana at approximately 422mg per medium fruit. A single day eating several of these consistently can meaningfully increase dietary potassium intake. Sustained improvement requires consistent eating patterns over weeks rather than a single high-potassium day, because the body regulates potassium tightly and excess is excreted rapidly. People on diuretics or other medications affecting potassium should discuss dietary changes with their GP.
ONE MORE THING BEFORE YOU GO If your symptom pattern is slightly different from what is described here, tell us in the comments. Tell us your three most persistent symptoms and how long they have been present. We read every comment and respond with what the research says about your specific picture. Muscle cramps and weakness without an obvious explanation are particularly worth mentioning. Potassium, magnesium, and calcium can all contribute and the combination differs from person to person. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are on medications that affect electrolyte levels or are experiencing significant symptoms, consult a qualified healthcare provider before self-managing potassium intake.
Never Miss any Updates From Blog!




No products in the cart.