Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article

If you are experiencing persistent muscle cramps, tingling in your hands or feet, or bones that feel increasingly fragile, the question of whether calcium intake is adequate is worth asking. The symptoms associated with low calcium are real. The biology behind them is also more nuanced than most sources present.
Your body maintains blood calcium within a very tight range. It does this partly by drawing calcium from bone when dietary intake is insufficient. This compensatory mechanism is effective in the short term. Sustained over months and years, particularly when combined with low vitamin D, which is required for calcium absorption in the gut, it has limits. The symptoms associated with insufficient calcium most commonly reflect the consequences of that sustained strain on both the bone reservoir and neuromuscular function.
This post explains the biology accurately, describes the symptoms that research associates with inadequate calcium intake, identifies who is most at risk, and explains how to assess and address the situation. It also explains what these symptoms share with other mineral deficiencies so you can distinguish between them.
BEFORE YOU READ FURTHER This post covers symptoms associated with inadequate calcium intake and the conditions that impair calcium absorption. These symptoms are non-specific and overlap significantly with other mineral deficiencies, particularly magnesium. The post describes associations supported by research, not direct causation. If you are experiencing severe muscle spasms, facial muscle twitching, an irregular heartbeat, or difficulty breathing, please seek emergency medical attention. Severe hypocalcaemia, a significant fall in blood calcium, requires immediate clinical treatment. If you are experiencing gradual muscle cramps, bone discomfort, or nerve tingling and are at risk for inadequate calcium or vitamin D intake, this post is written for your situation. Getting tested is the correct first step and this post explains what to ask for. |
This post addresses symptoms associated with chronically inadequate calcium and vitamin D intake, and the downstream effects on neuromuscular function and bone health in otherwise healthy adults.
It does not address clinical hypocalcaemia, which is a significant fall in blood calcium typically caused by hypoparathyroidism, severe vitamin D deficiency, renal disease, or other medical conditions requiring clinical diagnosis and treatment. Those presentations are medical emergencies or chronic conditions managed by clinicians, not by dietary adjustment.
The symptoms described here, muscle cramps, nerve tingling, and bone-related symptoms, overlap substantially with magnesium deficiency, potassium deficiency, and other conditions. This post names that overlap explicitly and recommends testing before attributing symptoms to calcium alone.
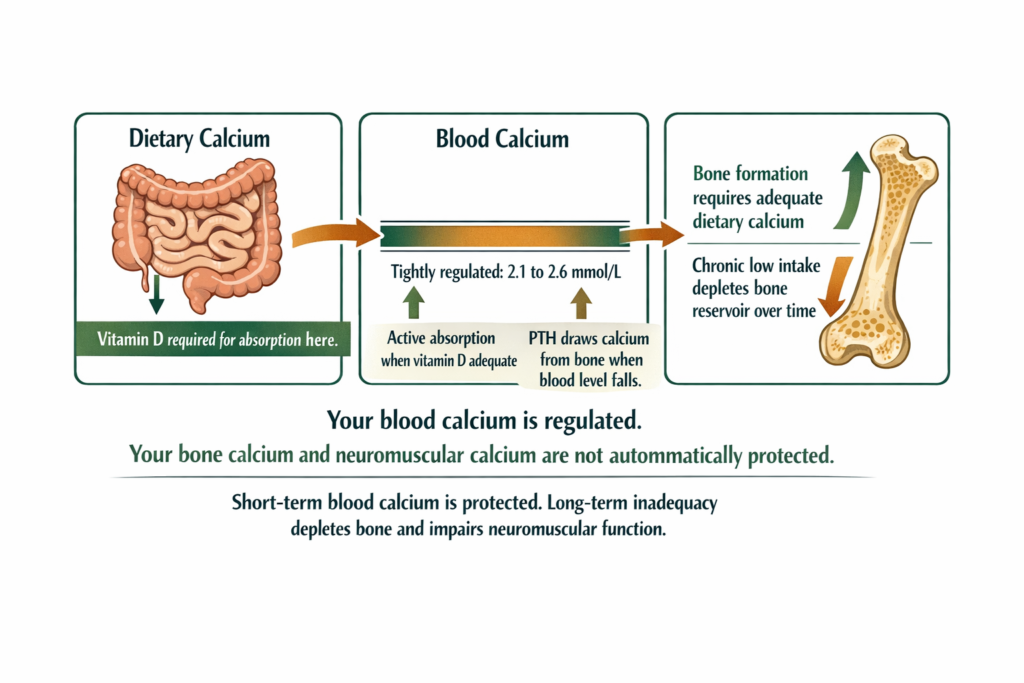
Calcium in the body is distributed between three compartments. Ninety-nine percent is stored in bones and teeth as hydroxyapatite. Approximately one percent circulates in the blood. A small fraction exists within cells and governs muscle contraction and nerve signalling.
Blood calcium is tightly regulated by parathyroid hormone (PTH) and vitamin D. When blood calcium falls, PTH signals the kidneys to retain calcium, the bones to release it, and the gut to increase absorption if vitamin D is present. This means blood calcium often remains within the normal range even when dietary intake is low, at least in the short term.
The consequence of relying on bone resorption to maintain blood calcium is gradual. Bone density falls. Over years, this increases fracture risk. The neuromuscular consequences of sustained low intake are less straightforward: muscle cramps, tingling, and nerve sensitivity are associated with low calcium states in the research literature, but the exact threshold and mechanism in mild dietary insufficiency are still debated. Severe falls in blood calcium produce clear neuromuscular symptoms. Mild, chronic, dietary insufficiency produces subtler effects that overlap with other mineral deficiencies (Peacock, 2010).
DEFINITION PARATHYROID HORMONE (PTH) A hormone produced by the parathyroid glands that governs calcium balance. When blood calcium falls, PTH is released. It signals three responses: the kidneys retain more calcium in urine, the bones release calcium into the blood, and the gut increases calcium absorption when vitamin D is present. PTH is why blood calcium often remains normal even when dietary intake is low. It is also why bone calcium is drawn down gradually over time when intake is consistently insufficient. Elevated PTH alongside low-normal blood calcium is a useful clinical signal of inadequate calcium intake. Testing PTH alongside serum calcium and vitamin D gives a more complete picture than serum calcium alone. |
This section appears near the top of the post deliberately. Testing before attributing symptoms to calcium is the correct sequence.
Serum calcium measures total blood calcium. A normal result does not rule out inadequate intake because PTH compensates by drawing from bone. Normal serum calcium with elevated PTH and low vitamin D is a common pattern in people with dietary insufficiency.
Vitamin D (25-hydroxyvitamin D) is essential to test because vitamin D deficiency is one of the most common reasons calcium is not absorbed from the gut, regardless of intake. If vitamin D is low, correcting it is the primary step. Calcium cannot be absorbed adequately without it.
Parathyroid hormone (PTH) is the most sensitive indirect marker of calcium adequacy. Elevated PTH with normal serum calcium and low vitamin D indicates the body is compensating for insufficient calcium through bone resorption. This is the picture most consistent with chronic low dietary intake in otherwise healthy people.
Ionised calcium measures the biologically active fraction of blood calcium. It is a more precise test used in clinical settings when total serum calcium is borderline or ambiguous.
Recommended daily intake for context: Adults aged 19 to 50 require approximately 1,000mg of calcium per day. Adults over 50, particularly postmenopausal women, require 1,200mg. These targets reflect the amount needed to minimise bone loss, not just avoid acute deficiency.
WHAT TO DO ABOUT IT Ask your GP for serum calcium, vitamin D (25-hydroxyvitamin D), and PTH together, not just serum calcium alone. The full picture, a normal serum calcium with elevated PTH and low vitamin D, is more clinically useful than any single result. If vitamin D is low, correcting it is the first priority because calcium absorption from the gut depends on it. If serum calcium is low, that requires clinical assessment rather than self-management. |
The symptoms below are associated with inadequate calcium in the research literature. They are not specific to calcium and overlap significantly with magnesium deficiency, potassium deficiency, and other conditions. The presence of these symptoms alongside dietary risk factors for calcium insufficiency makes calcium a candidate worth assessing. It does not confirm it.
Muscle cramps are not specific to calcium. They are equally associated with magnesium deficiency, potassium imbalance, dehydration, and nerve compression. Calcium becomes a stronger candidate when muscle cramps occur alongside tingling specifically around the mouth and in the hands and feet, when dietary calcium intake is consistently low, and when vitamin D is also insufficient. In that pattern, calcium and magnesium are both worth assessing.
The mechanism is real: calcium plays a direct role in muscle contraction and relaxation. When a nerve signal arrives at a muscle, calcium enters the cell and triggers contraction, then is pumped out to allow relaxation. In states of genuinely low blood calcium, neuromuscular excitability increases and muscles become more prone to involuntary firing. This is the mechanism behind clinical hypocalcaemia symptoms including cramps and spasms (Bushinsky and Monk, 1998). In mild dietary insufficiency where blood calcium stays normal through PTH compensation, the direct link is less clear and concurrent magnesium deficiency is often the more proximate driver.
Tingling around the mouth, in the hands, and in the feet is the most calcium-specific pattern in this cluster. It is still non-specific enough to share with other causes, but when it presents alongside the risk factors above, calcium status is the most important thing to test first.
DOES THIS APPLY TO YOU? Muscle cramps and tingling are among the most non-specific symptoms in this post. They are associated with low calcium but equally associated with low magnesium, low potassium, dehydration, nerve compression, and thyroid dysfunction. Calcium is one of several candidates to assess. Testing is the correct first step rather than supplementing based on symptoms alone. |
Bone effects are where the evidence for calcium is strongest and least contested. Reduced bone mineral density from sustained inadequate intake is a well-documented consequence supported by large-scale studies. Unlike the neuromuscular symptoms, which are shared across multiple deficiencies, bone resorption from chronic low calcium is relatively specific to calcium and vitamin D inadequacy in otherwise healthy adults. This presents as aching bone discomfort, increased fracture risk from minor trauma, and height loss in older adults.
Bone pain from other causes including vitamin D deficiency in isolation, osteoporosis from non-dietary causes, and inflammatory conditions should be excluded by a GP assessment. Bone density testing (DEXA scan) is the clinical method for assessment and is recommended for postmenopausal women and older adults with risk factors.
Fatigue and mood changes are among the least specific symptoms in this post. They are associated with virtually every mineral deficiency as well as thyroid dysfunction, depression, poor sleep, and anaemia. Calcium becomes a more plausible contributor to fatigue and mood specifically in premenopausal women with PMS, where calcium supplementation has shown benefit for mood symptoms in a randomised controlled trial (Thys-Jacobs et al., 1998). Outside that context, calcium is a possible contributor in a broader picture rather than a primary cause.
If fatigue and mood changes are your primary symptoms without muscle cramps, tingling, or bone-related symptoms, investigating vitamin D, iron, magnesium, and thyroid function is more likely to find the driver than calcium testing alone. These symptoms alone are not sufficient reason to attribute the picture to calcium.
DOES THIS APPLY TO YOU? Fatigue and mood changes are possible contributors in the context of low calcium and vitamin D, but they are not reliable indicators of calcium deficiency on their own. If these are your primary symptoms without muscle cramps, tingling, or bone-related symptoms, a broader assessment including thyroid function, iron, and magnesium is more likely to find the driver than calcium testing alone. |
Postmenopausal women. Oestrogen supports calcium retention in bone. After menopause, oestrogen falls and calcium loss from bone accelerates significantly. The requirement increases to 1,200mg per day. This group has the highest documented risk of calcium-related bone loss and the strongest evidence for supplementation benefit.
People who avoid dairy without replacing it. Dairy is the most calcium-dense common food. People who remove it without consistently replacing it through fortified plant milks, leafy greens, almonds, canned fish with bones, or tofu are at high risk of falling below adequate intake.
People with low vitamin D. Low vitamin D impairs calcium absorption from the gut regardless of intake. This is one of the most common compounding factors in apparent calcium inadequacy. Northern latitude residence, limited sun exposure, dark skin, and indoor working all increase vitamin D deficiency risk.
Older adults. Calcium absorption efficiency declines with age. The requirement increases. Dietary patterns may narrow. Kidney function affecting calcium regulation changes. All these factors converge in older adults.
People with malabsorption conditions. Coeliac disease, inflammatory bowel disease, and bariatric surgery all impair calcium absorption and increase deficiency risk significantly.
People on long-term corticosteroids. Corticosteroids reduce calcium absorption and increase bone resorption. Long-term use increases both calcium deficiency and osteoporosis risk.
The symptoms most commonly associated with calcium deficiency, muscle cramps, nerve tingling, and neuromuscular excitability, are almost identical to those associated with magnesium deficiency. This is not a coincidence.
Magnesium regulates the channels through which calcium enters and exits cells. Low magnesium causes calcium channels to become overactive. Paradoxically, low magnesium can produce symptoms of neuromuscular excitability that look identical to low calcium, sometimes even when calcium intake is adequate. When both are low, the symptoms compound. This is why addressing magnesium alongside calcium often produces better results than addressing either alone (Garrison et al., 2012).
The practical implication for anyone with muscle cramps and tingling: test and address both. Do not assume calcium is the primary driver without also considering magnesium. They are frequently co-depleted through the same dietary patterns, stress responses, and lifestyle factors.
How magnesium deficiency produces its own overlapping symptom cluster, and why magnesium and calcium must be addressed together for full neuromuscular recovery, is covered in our post on symptoms of magnesium deficiency and the cellular mechanism behind each one.
WHAT TO DO ABOUT IT Address calcium and magnesium together rather than sequentially. Both are required for normal neuromuscular function. Both deplete through similar dietary and lifestyle patterns. The foundation is dietary: consistent calcium-rich foods daily and magnesium-rich foods including nuts, seeds, and legumes. Vitamin D status must be adequate for calcium absorption to work. If supplementing, calcium citrate is better absorbed than calcium carbonate across different conditions. Do not take large doses of calcium and magnesium simultaneously as they compete for absorption at high amounts. Take calcium with food, ionic magnesium through the morning sipping protocol. |
Adults aged 19 to 50 need approximately 1,000mg of calcium per day. Adults over 50, and postmenopausal women specifically, need 1,200mg. These targets come from national dietary guidelines and represent the intake associated with minimising bone loss, not just preventing acute deficiency.
To put this in context: one 200ml glass of dairy milk provides approximately 240mg. One cup of cooked kale provides approximately 180mg. One 85g serving of canned sardines with bones provides approximately 325mg. A diet that consistently falls below these targets across multiple food groups over months is where the risk accumulates.
Vitamin D alongside calcium: the recommended daily intake for vitamin D is 400 to 800 IU for most adults, with many clinicians recommending higher levels for those with limited sun exposure. Without adequate vitamin D, calcium from food and supplements absorbs poorly regardless of intake amount.
Shilajit resin contains over 80 ionic trace minerals including magnesium, zinc, and potassium, alongside naturally occurring fulvic acid that enhances cellular mineral transport. While Shilajit is not a primary calcium source and does not replace dietary calcium or calcium supplementation for people with confirmed deficiency, it addresses the broader trace mineral environment that supports mineral metabolism. The mineral co-factor picture around calcium, particularly magnesium’s role in calcium channel regulation, is the area where Shilajit’s ionic mineral profile is most relevant.
Standard Thinking | The Biological Reality |
|---|---|
If my blood calcium is normal, my calcium status is fine | Blood calcium is tightly regulated by PTH and remains normal even when intake is low, at the cost of drawing from bone. Normal serum calcium alongside elevated PTH and low vitamin D indicates dietary insufficiency. The full picture requires all three markers |
Calcium is mainly about bone health | Bone health is the most well-evidenced long-term consequence of low intake. Calcium is also involved in muscle contraction, nerve signalling, and neurotransmitter release. The non-bone effects are real but more complex and less directly caused by mild dietary insufficiency than bone effects |
Muscle cramps mean I need calcium | Muscle cramps are associated with low calcium but equally associated with low magnesium, low potassium, dehydration, and other conditions. Calcium is one of several candidates. Testing both calcium and magnesium is the correct first step before supplementing either |
Drink milk and your calcium is covered | Dairy is a useful calcium source but absorption depends on vitamin D. Low vitamin D means calcium from food and supplements is poorly absorbed regardless of quantity. Both must be adequate for the system to function |
What are the symptoms of calcium deficiency?
The symptoms most consistently associated with inadequate calcium intake and low blood calcium include muscle cramps particularly in the legs and feet, tingling or numbness especially around the mouth and in the hands and feet, bone pain and increased fracture risk from sustained low intake, and in severe clinical cases, muscle spasms and irregular heartbeat. It is important to note that these symptoms are non-specific and overlap significantly with magnesium deficiency, potassium deficiency, and other conditions. The presence of these symptoms alongside dietary risk factors for low calcium intake is a reason to test, not a confirmed diagnosis.
Does low calcium cause muscle cramps?
Low blood calcium is associated with increased neuromuscular excitability and muscle cramps. In clinical hypocalcaemia, where blood calcium falls significantly, muscle cramps and spasms are a well-documented effect. In mild dietary insufficiency where blood calcium remains within the normal range through PTH compensation, the direct link to muscle cramps is less clear. Concurrent magnesium deficiency, which depletes through similar patterns and produces identical symptoms, is often a compounding factor. Addressing both together produces more consistent improvement than addressing calcium alone.
How do I know if my calcium is low?
Testing is more reliable than symptoms alone because low calcium symptoms overlap substantially with other deficiencies. Ask your GP for serum calcium, vitamin D (25-hydroxyvitamin D), and PTH together. Normal serum calcium with elevated PTH and low vitamin D indicates the body is compensating for dietary insufficiency through bone resorption. Vitamin D below 50 nmol per litre impairs calcium absorption and should be addressed as a priority. If serum calcium is below the reference range, that is a clinical finding requiring GP assessment and management rather than self-directed supplementation.
Can calcium deficiency cause anxiety?
Some research associates low calcium and vitamin D with mood changes, and calcium supplementation has shown benefit for premenstrual mood symptoms in controlled trials. However, the direct causal link between mild dietary calcium insufficiency and anxiety in otherwise healthy adults is not strongly established. If anxiety is a primary symptom, broader assessment including magnesium, vitamin D, iron, and thyroid function is more likely to identify the driver. Calcium is a possible contributor in the overall picture rather than a likely primary cause of anxiety in isolation.
How long does it take to improve calcium deficiency symptoms?
Neuromuscular symptoms such as cramps and tingling, when they are associated with calcium and magnesium insufficiency, typically begin improving within two to four weeks of consistent dietary improvement and supplementation alongside vitamin D correction. Bone effects take much longer: measurable improvements in bone density require months to years of sustained adequate intake. If testing confirms low vitamin D, correcting it first is often the most impactful step because it restores the gut absorption capacity that dietary calcium depends on.
ONE MORE THING BEFORE YOU GO If you have had blood calcium tested and it came back normal but symptoms persist, tell us in the comments. The testing picture, including vitamin D, ionised calcium, and parathyroid hormone, is more complex than a single serum result and we will address your specific situation directly. If you are unsure whether your symptoms are calcium, magnesium, or something else, describe the pattern and we will point you toward the most relevant post for your situation. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are experiencing severe muscle spasms, irregular heartbeat, or difficulty breathing, seek emergency medical attention. If blood calcium testing returns a low result, seek GP assessment before self-treating.
Never Miss any Updates From Blog!



No products in the cart.