Sleep Deprivation Symptoms: What Poor Sleep Is Actually Doing to Your Body and What to Do About It
The answer is not that your body is tired in a general sense. Each symptom on the list below has...
Read Article
You drink water constantly. Two litres. Sometimes three. You carry a bottle everywhere. You track it. You remind yourself. And yet by mid-afternoon you are exhausted, foggy, and somehow still thirsty. Your lips are dry. Your skin feels tight. Your urine is clear, which everyone says means you are hydrated, and still your body is sending distress signals you cannot explain.
You have searched for answers. You have been told to drink more. You have been told to add electrolytes. You have bought the powders, the tablets, the drinks. Some days it is slightly better. Most days the pattern repeats.
Our research indicates this is not a discipline problem. It is not a volume problem. It is a biological mechanism problem, and it has a precise explanation that your doctor was almost certainly never taught.
Before the mechanism, a brief check. Mark how many of these apply to you consistently, not occasionally.
You drink adequate water throughout the day and still feel thirsty, dry, or unrefreshed by the early afternoon.
Fatigue arrives reliably in the mid-afternoon regardless of how much sleep you had the night before.
Your thinking feels slower and less clear in the second half of the day. Finding words, concentrating, and retaining information all require more effort.
Your skin feels tight or dry despite drinking plenty of water. Moisturiser helps temporarily but does not solve it.
You experience muscle cramps or twitching particularly at night, not during exercise.
Your urine is consistently clear suggesting you are consuming adequate water, but the symptoms above persist regardless.
If you recognise three or more of these consistently, the pattern is almost certainly cellular rather than volumetric. The mechanism below explains precisely why drinking more water will not resolve it.
BEFORE YOU READ FURTHER This post describes one specific mechanism behind the symptoms above: intracellular dehydration driven by mineral depletion and reduced sodium-potassium pump efficiency. This is a real and documented mechanism. It is not the only mechanism that produces fatigue, brain fog, or persistent thirst. See a healthcare provider before treating this as a cellular hydration issue if: symptoms appeared suddenly rather than gradually, fatigue is severe and significantly affecting your daily function, you have a diagnosed kidney condition, diabetes, or cardiovascular condition, or you are taking medications that affect fluid or electrolyte balance. The mechanism described in this post is most relevant for people experiencing a gradual, persistent, multi-symptom pattern without a diagnosed underlying condition. If that is your situation, read on. |
Most people experiencing this pattern are living with what the biological literature describes as cellular dehydration: a state in which adequate water is consumed but insufficient water is reaching the inside of the cells where it is actually needed.
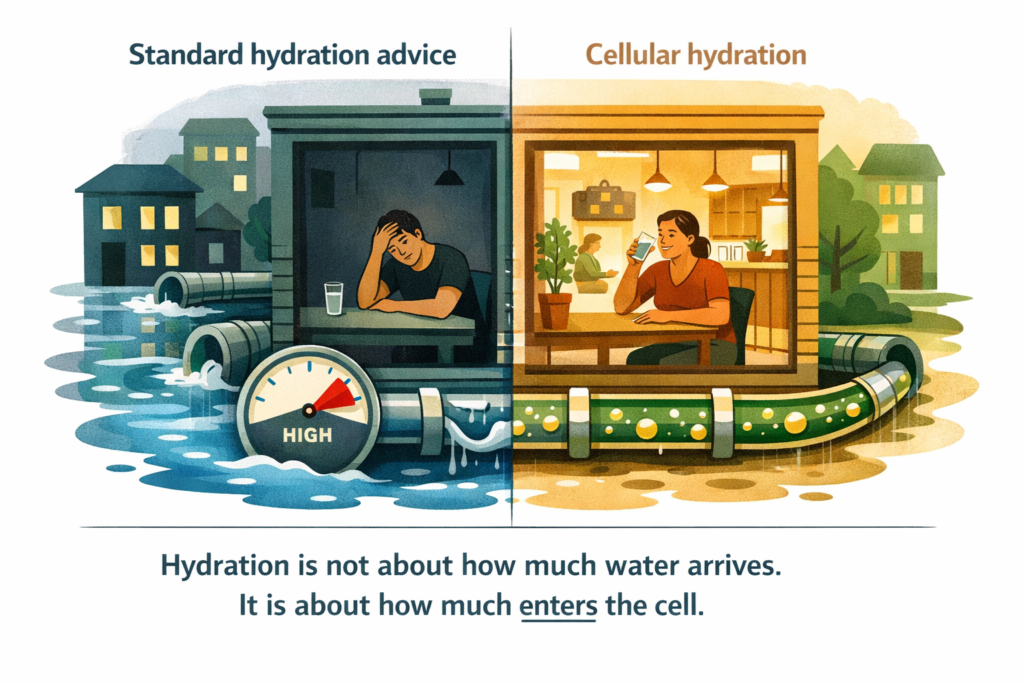
Your body is not one container. It is approximately 37 trillion individual containers, each requiring water to function. The question is never just whether water reached your stomach. The question is whether water crossed the cell membrane and entered the cell itself. Those are two entirely different biological events, separated by a mechanism that most hydration advice completely ignores.
Think of it this way. You can flood a city with water. But if the pipes leading into individual buildings are blocked or unpowered, the buildings stay dry regardless of how much water is in the streets. Cellular dehydration symptoms persist not because there is no water, but because the delivery system into the cell has failed.
DEFINITION CELLULAR DEHYDRATION A state in which adequate water is consumed but insufficient water reaches the inside of cells where it is biologically needed. Caused by reduced efficiency of the aquaporin channels that control water entry into cells, which depend on the sodium-potassium pump to function. Distinct from volumetric dehydration, which is simply insufficient fluid intake. Standard hydration advice addresses volumetric dehydration. It does not address cellular dehydration. |
WHAT TO DO ABOUT IT Understanding the distinction between volumetric and cellular dehydration changes the intervention. If the problem is volumetric, drink more water. If the problem is cellular, restore the mineral supply that powers the sodium-potassium pump and opens the aquaporin channels. The volume of water you are drinking is almost certainly not the variable that needs to change. |
DOES THIS APPLY TO YOU? If drinking more water produces more frequent urination but no meaningful improvement in your fatigue, mental clarity, or persistent thirst, you are almost certainly in the cellular rather than volumetric dehydration pattern. If increasing water intake makes the symptoms worse rather than better, the dilution of remaining ionic minerals is likely compounding the pump depletion. If symptoms appeared alongside a change in your water source such as moving to RO filtered water or a new area, the mineral change is the most likely trigger. |
Water does not pass freely through cell walls. It enters through dedicated protein channels called aquaporins, discovered by Peter Agre in 1992, for which he received the Nobel Prize in Chemistry in 2003 (Agre, 2004). These channels are not permanently open. They open and close in response to specific electrochemical conditions on either side of the cell membrane.
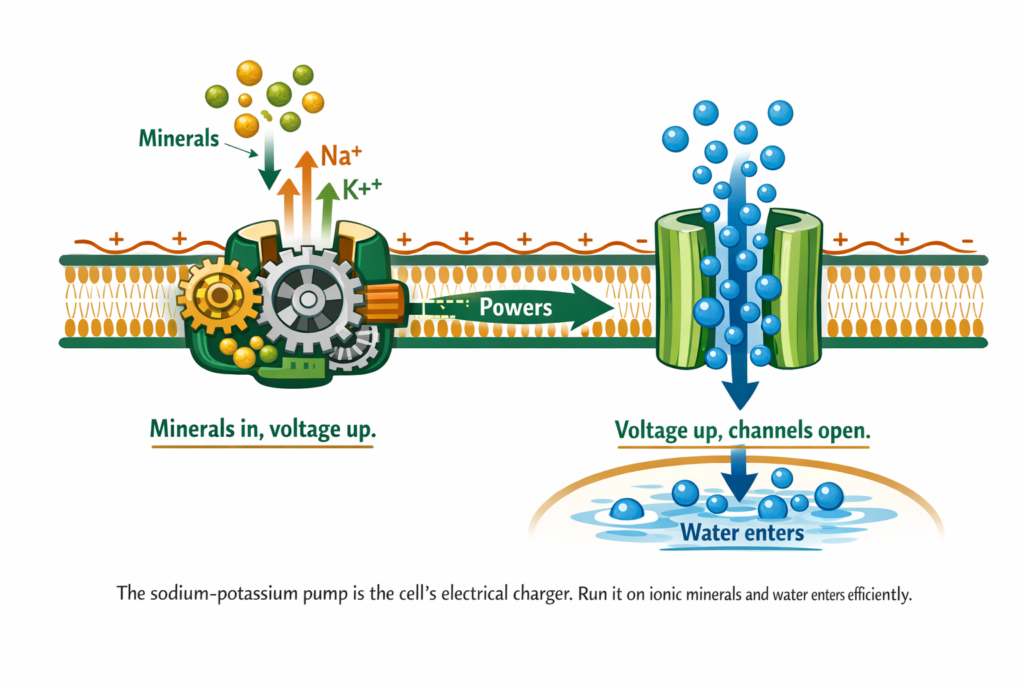
Those electrochemical conditions are created and maintained by the sodium-potassium pump, a protein engine embedded in every cell membrane that pushes sodium ions out and pulls potassium ions in, thousands of times per second. This constant exchange generates a voltage across the membrane, the same basic principle that powers a battery. That voltage is what signals the aquaporin channels to open (Skou, 1997).
Run the sodium-potassium pump continuously and the cell stays charged, the aquaporin channels stay open, and water enters efficiently. Deplete the minerals that power it and the pump slows, the voltage drops, and the channels close. Water continues arriving at the cell. It simply stops getting in.
DEFINITION AQUAPORINS Protein channels embedded in cell membranes that control water entry into cells. Discovered by Peter Agre, Nobel Prize in Chemistry 2003. Aquaporins do not remain permanently open. They open in response to the electrochemical voltage generated by the sodium-potassium pump. When the pump runs below capacity due to mineral depletion, aquaporin channels partially close and water entry into the cell is reduced regardless of how much water is consumed. |
WHAT TO DO ABOUT IT The minerals that power the sodium-potassium pump are not generic supplements. They are ionic minerals: sodium, potassium, magnesium, calcium, and a spectrum of trace minerals in their dissolved, electrically charged state. Not particles. Not powder. Dissolved ions in the same form found naturally in mineral-rich water that has moved through geological formations over centuries. Restoring this ionic mineral supply restores pump efficiency and reopens aquaporin channels. |
DOES THIS APPLY TO YOU? If your symptoms are worst in the afternoon and early evening rather than constant throughout the day, this reflects the daily depletion pattern. The pump has been running since you woke up, consuming ionic mineral reserves without adequate replenishment. By mid-afternoon the reserves are at their lowest and cellular hydration is at its worst. If this timing pattern fits your experience, the pump depletion mechanism is almost certainly the driver. |
If the problem is a depleted sodium-potassium pump, adding more water does not solve it. It is the biological equivalent of pouring more petrol near an engine with no ignition. The fuel is present. The mechanism to use it is offline.
This is the precise reason why drinking water but still dehydrated is not a contradiction. It is a diagnosis. The body is receiving water and losing it through normal kidney processing without it completing the journey into the cells where it is needed. The kidneys do their job. The cells do not get served.
Our research indicates this pattern is worsened significantly by the water most households are drinking today. Reverse osmosis filtered water, sold as the gold standard of drinking water safety, delivers water at 10 to 50 parts per million total dissolved solids. Natural water that the human body evolved drinking was 200 to 400 parts per million, carrying a full spectrum of ionic minerals the sodium-potassium pump requires.
The filtration removed the contaminants. It also removed the mineral supply that powers cellular hydration. The water is clean. From the cell’s perspective, it is also empty.
According to the World Health Organization, low mineral water increases urinary excretion of sodium, potassium, magnesium, and calcium, compounding the depletion rather than correcting it (Kozisek, 2005). You drink mineral-depleted water. It draws more minerals out. The pump runs slower. Fewer aquaporin channels open. Less water enters the cells. You drink more water. The cycle continues.
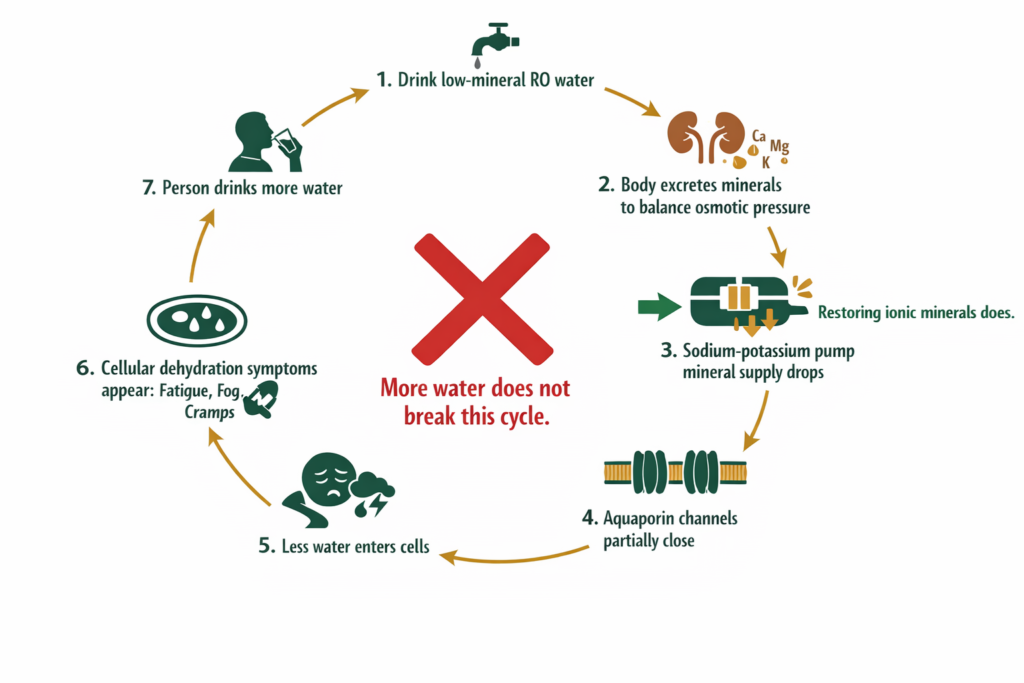
WHAT TO DO ABOUT IT Breaking the cycle requires addressing the mechanism at Step 3, not adding more volume at Step 7. Restore the ionic mineral supply to the sodium-potassium pump. The pump recovers efficiency. Aquaporin channels reopen. Water enters the cells. The thirst signal switches off because the biological need has been met, not because you drank past the signal. |
DOES THIS APPLY TO YOU? If you drink RO filtered water as your primary water source and have done so for more than six months, mineral depletion from your water source is almost certainly a contributing factor to your symptoms. Test your water with a TDS meter: a reading below 100 PPM confirms the water is providing minimal ionic mineral supply to the pump. If your water reads above 200 PPM and symptoms persist, the water is not the primary driver and the mineral depletion is coming from another source such as chronic stress, high caffeine intake, or exercise without mineral replenishment. |
The following are not random health complaints. They are the predictable output of a sodium-potassium pump running below capacity on mineral-depleted water.
Persistent thirst after drinking. The thirst signal originates in the hypothalamus in response to osmotic pressure changes in the blood. When water is not entering cells efficiently, osmotic pressure remains dysregulated despite fluid intake. The thirst signal does not switch off because the biological need has not been met (Popkin et al., 2010).
Afternoon energy collapse. The sodium-potassium pump consumes approximately 20 to 40 percent of total cellular energy in active tissues. When it is running below capacity, cellular energy production drops measurably. This manifests as fatigue that arrives reliably in the afternoon regardless of sleep quality.
Brain fog and difficulty concentrating. Neurons are among the most electrically active cells in the body and among the most sensitive to aquaporin channel disruption. Cognitive performance correlates directly with neuronal hydration status. A partially closed aquaporin channel does not stop a neuron from firing. It slows and weakens the signal (Papadopoulos and Verkman, 2013).
Night cramps and muscle twitching. Muscle contraction and release depend on precise sodium-potassium ratios across muscle cell membranes. When those ratios drift due to pump underperformance, the electrical signals controlling muscle function become erratic. This appears most noticeably at night when dietary mineral intake has stopped and the pump is running on reserves.
Dry skin despite adequate water intake. Skin cells follow the same aquaporin pathway as every other cell. Mineral-depleted water does not hydrate skin cells more effectively than it hydrates cells elsewhere in the body (Verdier-Sevrain and Bonte, 2007).
WHAT TO DO ABOUT IT The intervention for each of these symptoms is the same: restore the ionic mineral supply the sodium-potassium pump requires to run at full capacity. This means ionic minerals in their dissolved, electrically charged state rather than mineral particles or powder forms that require digestion before use. The morning sipping protocol, dissolving ionic minerals in a one-litre bottle and sipping from waking until approximately 2pm, delivers a consistent supply through the hours of highest pump demand. |
DOES THIS APPLY TO YOU? If you recognise three or more of these symptoms and your water source is RO filtered or very low TDS, the mechanism fits precisely. If you recognise the symptoms but your water TDS is above 200 PPM, the mineral depletion is coming from elsewhere: chronic stress through the cortisol-mineral depletion pathway, high caffeine or alcohol intake increasing urinary mineral excretion, or sustained physical or cognitive exertion without replenishment. The symptoms are the same regardless of the depletion source. The solution is the same. The cause context helps you address both the symptom and the driver. |
This is not a criticism of medicine. It is an observation about what medicine measures and what it does not. Standard blood panels test serum electrolyte levels: the concentration of minerals in your blood. They do not measure intracellular mineral concentration, which is where the relevant depletion is occurring.
A person can have normal serum sodium and potassium levels while experiencing significant intracellular mineral depletion and correspondingly poor sodium-potassium pump performance. The gap between what is normal on a blood test and what is optimal at the cellular level is where most chronic low-grade health complaints live. Not sick enough for a diagnosis. Not well enough to feel the way biology is capable of making you feel.
Our research indicates this is precisely why the pattern of drinking water but still dehydrated is so consistently dismissed. It does not show up clearly on the tests available in a standard clinical setting. It shows up in how you feel every afternoon.
WHAT TO DO ABOUT IT A normal blood electrolyte panel tells you the compensatory mechanism is holding, not that intracellular mineral status is optimal. The most practical diagnostic approach outside specialist testing is the empirical trial: restore ionic mineral supply for two to four weeks using a full-spectrum ionic source and observe whether the symptom pattern responds. Resolution of symptoms is itself the most direct evidence that cellular mineral depletion was the driver. |
DOES THIS APPLY TO YOU? If you have been told your blood electrolytes are normal and have therefore concluded that minerals are not your issue, that conclusion was based on a serum measurement of the compensated compartment. Normal serum electrolytes mean your body is successfully drawing from intracellular stores to maintain blood levels. They do not tell you whether those intracellular stores are adequate. If your symptom pattern fits what is described in this post, the serum test result is not contradictory. It is consistent with the mechanism. |
If this were real, doctors and nutritionists would be talking about it. The fact that they are not suggests it is overstated.
The mechanism is not disputed. The Nobel Prize-winning discovery of aquaporins, the sodium-potassium pump described in every cell biology textbook, the WHO documentation of mineral loss from low TDS water: none of this is fringe science. It is undergraduate physiology.
What is not widely communicated is the practical implication of combining this established mechanism with the widespread adoption of reverse osmosis filtration over the past three decades. The mechanism was established before RO filtration became a household product. The downstream consequence for daily hydration was never joined up into public health guidance.
This is not suppression. It is the normal lag between basic science and practical application. The research exists. The communication of its implications to the general public has not caught up.
Restoring cellular hydration requires addressing the mechanism, not the volume. Three steps in sequence.
Step one: Identify your water’s TDS. A basic TDS meter costs under five Australian dollars and takes thirty seconds to use. A reading of 10 to 50 PPM confirms your water is mineral-depleted. A reading below 100 PPM means the sodium-potassium pump is not receiving adequate mineral supply from your water source.
Step two: Restore ionic minerals, not just any minerals. The form matters as much as the quantity. Ionic minerals are single electrically charged atoms fully dissolved in water, the form the sodium-potassium pump recognises directly. Most commercial electrolyte products add two or three minerals in non-ionic form at concentrations too low to meaningfully restore pump function. A full-spectrum ionic mineral source that includes naturally occurring fulvic acid as the cellular transport mechanism is the complete solution.
Step three: Verify the restoration. Use your TDS meter to confirm your restored water reaches 150 to 300 PPM. Below 150 PPM and the mineral supply remains insufficient. Above 300 PPM from a supplemental source and you are adding more than the body needs. The 150 to 300 PPM range is the biological target.
The full mechanism behind TDS ranges and what each means biologically is covered in our post on what your water TDS reading actually means for cellular hydration.
Standard Thinking | The Biological Reality |
|---|---|
Drink more water to fix dehydration | Restore the mineral supply that opens the aquaporin channels. Volume is not the variable. The delivery mechanism is. |
Clear urine means you are hydrated | Clear urine means water passed through efficiently. It does not mean water entered your cells. The kidneys processed the water. The cells may not have received it. |
Electrolyte powders solve mineral depletion | Most electrolyte products add two or three minerals in non-ionic form at insufficient concentration to meaningfully restore sodium-potassium pump function. |
RO filtered water is the healthiest choice | RO water is the safest choice for contaminant removal. It is not the most biologically complete choice. The filtration that removed contaminants also removed the ionic mineral supply the pump requires. |
Persistent thirst means drink more | Persistent thirst after adequate fluid intake means water is not reaching your cells. The thirst signal is responding to osmotic pressure dysregulation, not to volume deficit. |
Your doctor would know if something was wrong | Subclinical cellular dehydration does not appear on standard blood panels. Serum electrolytes measure the compensated compartment. They do not measure intracellular mineral status where the relevant depletion occurs. |

Fatigue that does not resolve with sleep and does not resolve with increased water intake is a recognised pattern of poor cellular hydration. The sodium-potassium pump consumes 20 to 40 percent of total cellular energy in active tissues. When it is running below capacity on mineral-depleted water, the energy deficit it creates compounds through the day independently of sleep. Sleep restores neurological function. It does not restore the ionic mineral supply the pump needs to run at full capacity.
During sleep, the body continues cellular maintenance processes that consume ionic minerals without any dietary replenishment. By morning, after 7 to 8 hours without mineral intake, the sodium-potassium pump is running on its lowest mineral reserves of the day. If your water during the day was mineral-depleted, those reserves were already low before sleep. Waking up dehydrated despite drinking throughout the previous day is a reliable indicator of insufficient ionic mineral intake rather than insufficient water volume.
The thirst mechanism is triggered primarily by blood osmolality changes sensed in the hypothalamus. In chronic cellular dehydration driven by mineral depletion rather than volume deficit, blood osmolality can remain within a range that does not strongly trigger thirst, while intracellular dehydration continues. This is why normal or suppressed thirst does not rule out cellular dehydration. The symptom pattern, fatigue, brain fog, dry skin, and muscle cramps, is a more reliable indicator than thirst signal alone.
The primary causes are: mineral-depleted drinking water reducing sodium-potassium pump efficiency, particularly reverse osmosis filtered water at 10 to 50 PPM total dissolved solids; high intake of diuretic substances such as caffeine and alcohol that accelerate mineral excretion; prolonged physical or cognitive exertion depleting ionic mineral reserves faster than they are replenished; and chronic stress through the cortisol pathway which depletes magnesium and zinc with each activation. These causes often operate simultaneously, which is why the pattern is persistent rather than episodic.
You were not doing it wrong. You were following advice built on an incomplete model of how water actually enters the human cell. The eight glasses a day guidance addresses volume. It says nothing about the electrochemical conditions required to move that water from the space outside your cells to the space inside them, where it is biologically relevant.
The sodium-potassium pump is running. The aquaporin channels are waiting. The question is whether the water you are giving your body carries what is needed to open them.
Our research indicates it almost certainly does not. And the fix is not more water. It is better water.
ONE MORE THING BEFORE YOU GO If you have measured your water TDS and found something unexpected, or if you recognise the symptom pattern described here but something in your situation does not quite fit the mechanism we have described, leave it in the comments below. We read every comment and respond with what the research says. Tell us your TDS reading, your three most persistent symptoms, and how long you have been experiencing them. That is enough for us to give you a direct and useful response. |
Legal Disclaimer
The information in this post reflects Penantia’s interpretation of available scientific research and is intended for educational purposes only. It does not constitute medical advice, diagnosis, or treatment. If you are experiencing persistent fatigue, muscle cramps, or other health symptoms, consult a qualified healthcare provider.
Never Miss any Updates From Blog!




No products in the cart.